By Jeffrey Mark Taylor
Humans do not have continuous dielectric properties throughout their head/body, tissue/bone layers. Yet the FCC only requires SAR models/dummies (3-D phantoms) that are merely containers with a SINGLE frequency dependent dielectric fluid matching the mean dielectric properties of the head or body. (These are of a 6’2” 220 lbs. male originally done in the 50's utilizing “average” military personnel as result of military radio operator’s high disability/mortality rates). Finally, the device manufacturers, currently required by the FCC to use this simplistic inaccurate modeling has little to do with the devices safety, rather instead a general heat output within the near field of these devices. For example, human skulls (and other human bones) act as antennas, conductors and reflectors of electromagnetic radiation - with capabilities varying with their chemistry, size and profiles (their biophysics). While human eyes are even more transparent to the microwave spectrum than to the visible spectrum (by their ability to penetrate closed irises & lids) which leaves varying directional dependent ways for radiation to enter without significant losses - and then not necessarily exiting; otherwise therefore left fully absorbed. This leaves varying hot spots in areas of the brain not showing up on the simplistic, voxel heat maps created from the SAR data streams when using only a device to ear approach, large heads/bodies, and mono-dielectric single layered fluid modeling used for portable (carried) devices' FCC grants of equipment authorizations (GEAs). For instance, when a subject uses one device/transmitter for listening/speaking, another for texting/surfing, and concurrently when other devices remain powered on by one's bed/crib-stand(s)/desks, extra radiation can blanket the entire body (or bodies - see previous 2 blogs below). These common multiple-use habits made without considering the other people/devices around discount the long-term health impacts of highly attenuated far-field radiation effects often occurring during the time the body and mind should instead be healing from the daily onslaughts of life. Another important FCC SAR weakness to be considered is that size (in this case) matters, leaving smaller bodies and heads (i.e. women or children) significantly more vulnerable to overheating and cell death (necrosis) than the body/head that the FCC's standard phantom and modeling technique represents (see 2nd Scribd study at the end of this blog entry). This approach has significant accuracy weaknesses w/o the decreasing of the voxel and phantom sizes coupled to the changing of the dielectric characteristics that more accurately represent the young developing brain. Finally, the current 2001 FCC thermal standards also imply that there is really only one form of health impact occurring because of the use of these devices’ radiation-THERMAL-cell death by heating-necrosis/electrocution (as now used in killing skin cancers)! However, some impacts not EVEN considered are the long-term effects occurring with as little as seven magnitudes less powerful than currently permitted. While the physicist may consider there to be a be dramatic danger difference between the activity of ionizing radiation or molecular vibrations, the biophysicist knows our bodies work changing their chemistry primarily instead, in small steps/cycles with little power by numerous catalyzed reactions. (Please see the blog titled further down from this link "Scientific evidence contradicts findings and assumptions of Canadian Safety Panel 6: Microwaves Act Through Voltage Gated Calcium Channel Activation to Induce Biological Impacts at Non-thermal Levels, Supporting a Paradigm Shift for Microwave/Lower Frequency Electromagnetic Field Action'
Further, we have to consider MORE what is happening medically in long-term exposures in adults (the mechanisms) that create the multiple symptoms we find in the individuals who are profoundly disabled by RFR exposures. Below, in the last full text study, Dr. Gunnar Heuser shows some significant differences in the brains of patients suffering from what he terms as "Electrohypersensitivity" (EHS) -usually defined instead as instead as- Electromagnetic Hypersensitivity sufferers who often have sensitivities more than 7 magnitudes lower than current FCC SAR standards, including their significant effects in the far field - MPE standards). Dr. Heuser uses a functional MRI medical diagnostic imaging technique, which is a way of showing resting state blood oxygenation abnormality in in the various brain component areas by magnetically spinning all the brain tissue water's hydrogen atoms and creating a 3-D micro-dot matrix soft tissue image using the probabilistic measurement electromagnetic field spin direction overlaying a 3-D MRI heat map of resting state blood oxygenation levels to the parts so defined by the brain image. This implies there is now an “objective”, treatment, “success”, verification. For example, in a hypothetical “success”, one treats a patient which this diagnostic fMRI had showed these characteristic EHS abnormalities with hyperbaric oxygen and after treatment the same EHS abnormalities then disappear or are greatly minimized. The obvious problem, however is Dr. Heuser is only treating/considering the electric field by his definition of EHS, which seems to ignore the possible effects of the magnetism on the diagnostics of his patients, simply because they have been essentially eliminated by dropping the magnetic from ElectroMAGNETIC Hypersensitivity. Unfortunately, however most EHS sufferers experience debilitating pain during MRI procedures and will not inflict that on themselves w/o more treatment successes, thereby avoiding the need for the DANGEROUS diagnostic procedure prescriptively.
Therefore, the current 2001 SAR power standards need to be appropriately modified & lowered (just like mileage was for automobiles during the oil crisis) as SAR modeling remains the most accurate one in near field conditions that personal devices (portable) are most often used in and we are in the throes of an EHS crisis. We can no longer afford to wait for the long-term studies showing linkages generations later as happened in cigarettes, asbestos etc.! Finally, please view my illuminating short study near the bottom of the Feb 2017 blog titled & here as a hotlink at: What Happens With Smartmeters When Installed in Condos? Thus for example when one reads one's smart meter (for some reason classified as a permanently located mobile device) regularly waiting several minutes for just one data readout- BEWARE, YOU DON'T EVEN HAVE TO BE NEXT TO THE METER ! THE ANTENNA ARE ALSO THE POWER WIRES SURROUNDING YOU INSIDE YOUR WALLS !
Humans do not have continuous dielectric properties throughout their head/body, tissue/bone layers. Yet the FCC only requires SAR models/dummies (3-D phantoms) that are merely containers with a SINGLE frequency dependent dielectric fluid matching the mean dielectric properties of the head or body. (These are of a 6’2” 220 lbs. male originally done in the 50's utilizing “average” military personnel as result of military radio operator’s high disability/mortality rates). Finally, the device manufacturers, currently required by the FCC to use this simplistic inaccurate modeling has little to do with the devices safety, rather instead a general heat output within the near field of these devices. For example, human skulls (and other human bones) act as antennas, conductors and reflectors of electromagnetic radiation - with capabilities varying with their chemistry, size and profiles (their biophysics). While human eyes are even more transparent to the microwave spectrum than to the visible spectrum (by their ability to penetrate closed irises & lids) which leaves varying directional dependent ways for radiation to enter without significant losses - and then not necessarily exiting; otherwise therefore left fully absorbed. This leaves varying hot spots in areas of the brain not showing up on the simplistic, voxel heat maps created from the SAR data streams when using only a device to ear approach, large heads/bodies, and mono-dielectric single layered fluid modeling used for portable (carried) devices' FCC grants of equipment authorizations (GEAs). For instance, when a subject uses one device/transmitter for listening/speaking, another for texting/surfing, and concurrently when other devices remain powered on by one's bed/crib-stand(s)/desks, extra radiation can blanket the entire body (or bodies - see previous 2 blogs below). These common multiple-use habits made without considering the other people/devices around discount the long-term health impacts of highly attenuated far-field radiation effects often occurring during the time the body and mind should instead be healing from the daily onslaughts of life. Another important FCC SAR weakness to be considered is that size (in this case) matters, leaving smaller bodies and heads (i.e. women or children) significantly more vulnerable to overheating and cell death (necrosis) than the body/head that the FCC's standard phantom and modeling technique represents (see 2nd Scribd study at the end of this blog entry). This approach has significant accuracy weaknesses w/o the decreasing of the voxel and phantom sizes coupled to the changing of the dielectric characteristics that more accurately represent the young developing brain. Finally, the current 2001 FCC thermal standards also imply that there is really only one form of health impact occurring because of the use of these devices’ radiation-THERMAL-cell death by heating-necrosis/electrocution (as now used in killing skin cancers)! However, some impacts not EVEN considered are the long-term effects occurring with as little as seven magnitudes less powerful than currently permitted. While the physicist may consider there to be a be dramatic danger difference between the activity of ionizing radiation or molecular vibrations, the biophysicist knows our bodies work changing their chemistry primarily instead, in small steps/cycles with little power by numerous catalyzed reactions. (Please see the blog titled further down from this link "Scientific evidence contradicts findings and assumptions of Canadian Safety Panel 6: Microwaves Act Through Voltage Gated Calcium Channel Activation to Induce Biological Impacts at Non-thermal Levels, Supporting a Paradigm Shift for Microwave/Lower Frequency Electromagnetic Field Action'
Further, we have to consider MORE what is happening medically in long-term exposures in adults (the mechanisms) that create the multiple symptoms we find in the individuals who are profoundly disabled by RFR exposures. Below, in the last full text study, Dr. Gunnar Heuser shows some significant differences in the brains of patients suffering from what he terms as "Electrohypersensitivity" (EHS) -usually defined instead as instead as- Electromagnetic Hypersensitivity sufferers who often have sensitivities more than 7 magnitudes lower than current FCC SAR standards, including their significant effects in the far field - MPE standards). Dr. Heuser uses a functional MRI medical diagnostic imaging technique, which is a way of showing resting state blood oxygenation abnormality in in the various brain component areas by magnetically spinning all the brain tissue water's hydrogen atoms and creating a 3-D micro-dot matrix soft tissue image using the probabilistic measurement electromagnetic field spin direction overlaying a 3-D MRI heat map of resting state blood oxygenation levels to the parts so defined by the brain image. This implies there is now an “objective”, treatment, “success”, verification. For example, in a hypothetical “success”, one treats a patient which this diagnostic fMRI had showed these characteristic EHS abnormalities with hyperbaric oxygen and after treatment the same EHS abnormalities then disappear or are greatly minimized. The obvious problem, however is Dr. Heuser is only treating/considering the electric field by his definition of EHS, which seems to ignore the possible effects of the magnetism on the diagnostics of his patients, simply because they have been essentially eliminated by dropping the magnetic from ElectroMAGNETIC Hypersensitivity. Unfortunately, however most EHS sufferers experience debilitating pain during MRI procedures and will not inflict that on themselves w/o more treatment successes, thereby avoiding the need for the DANGEROUS diagnostic procedure prescriptively.
Therefore, the current 2001 SAR power standards need to be appropriately modified & lowered (just like mileage was for automobiles during the oil crisis) as SAR modeling remains the most accurate one in near field conditions that personal devices (portable) are most often used in and we are in the throes of an EHS crisis. We can no longer afford to wait for the long-term studies showing linkages generations later as happened in cigarettes, asbestos etc.! Finally, please view my illuminating short study near the bottom of the Feb 2017 blog titled & here as a hotlink at: What Happens With Smartmeters When Installed in Condos? Thus for example when one reads one's smart meter (for some reason classified as a permanently located mobile device) regularly waiting several minutes for just one data readout- BEWARE, YOU DON'T EVEN HAVE TO BE NEXT TO THE METER ! THE ANTENNA ARE ALSO THE POWER WIRES SURROUNDING YOU INSIDE YOUR WALLS !
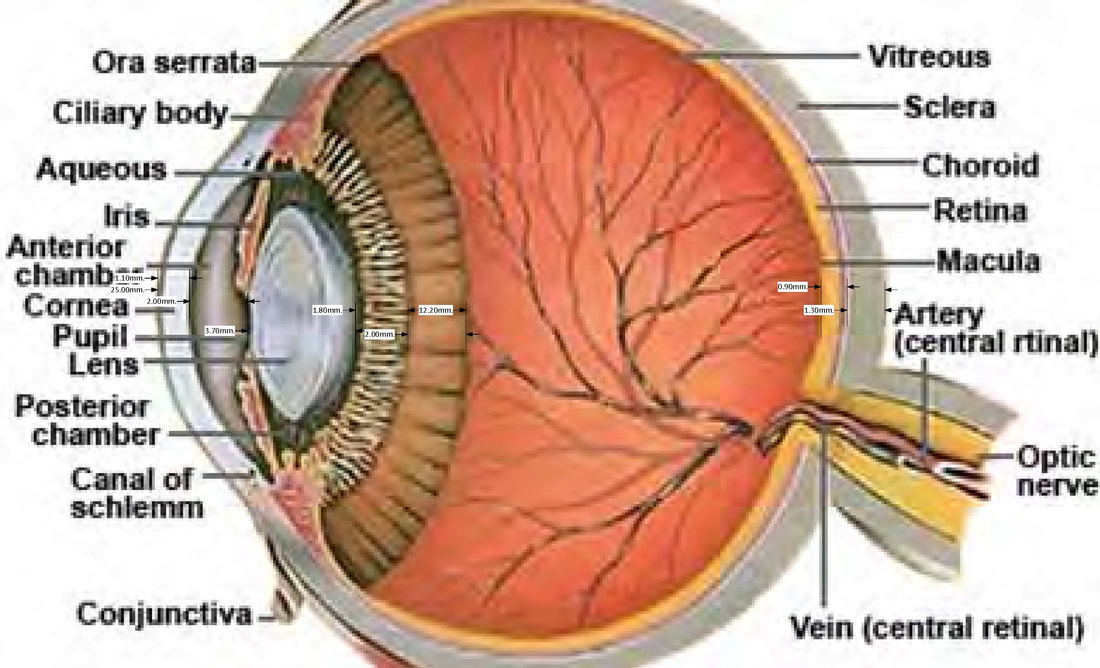
The human eye and some typical dielectric layer measurements
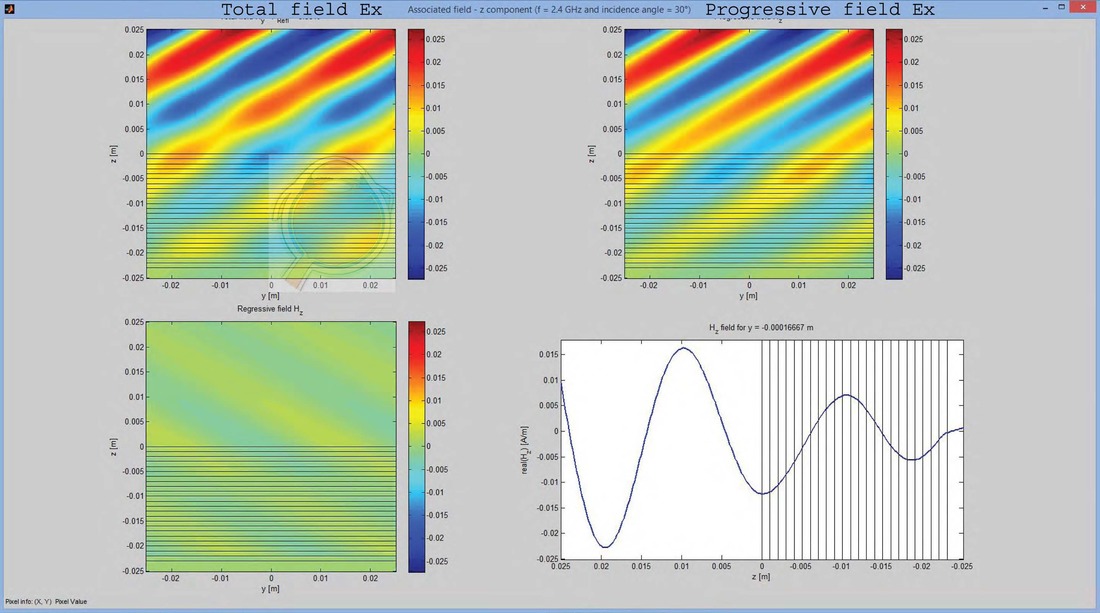
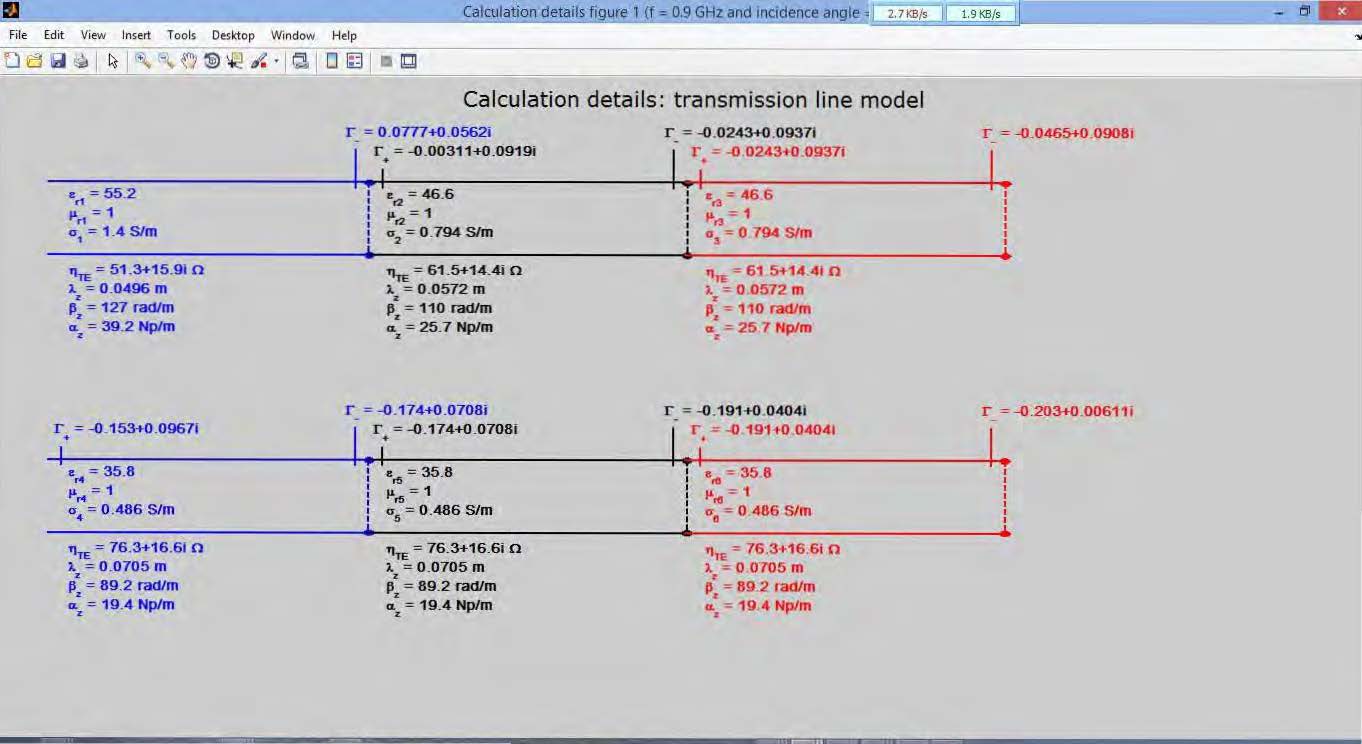
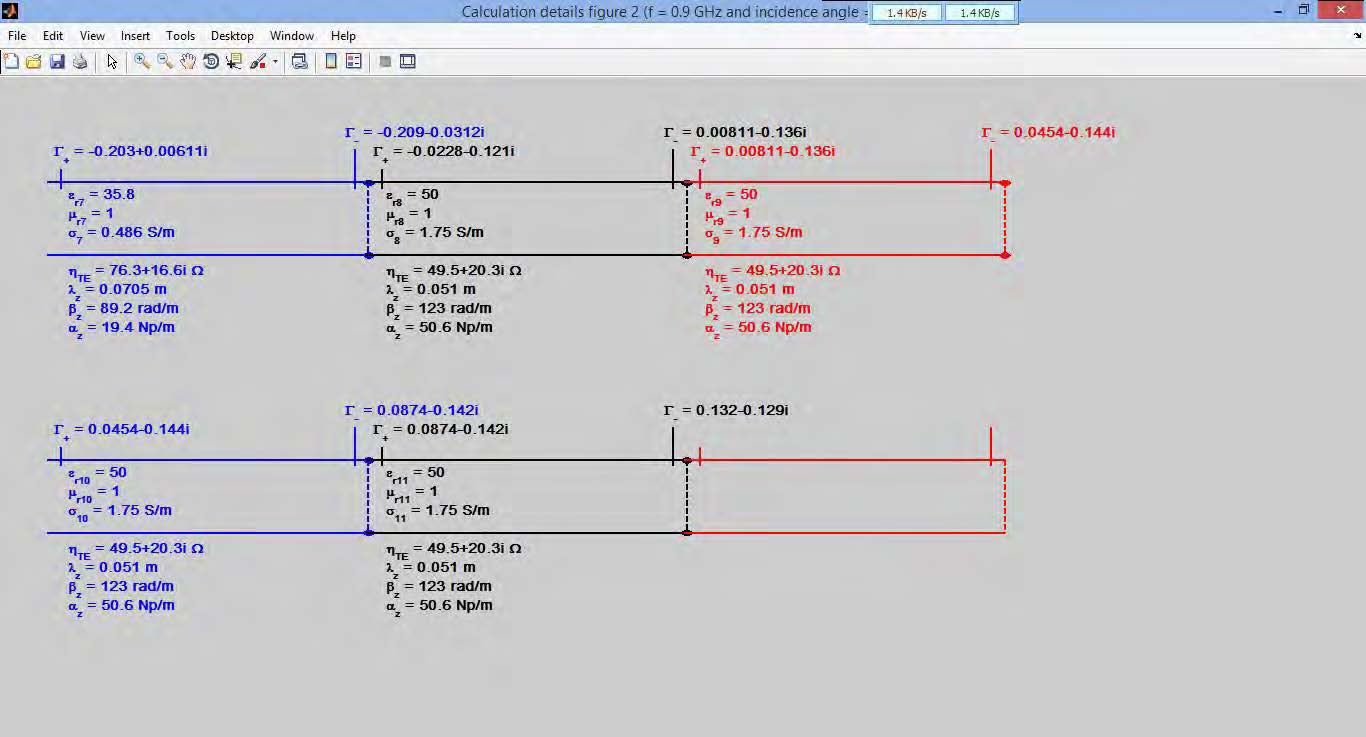
Using MatLab 2014b and Lorenzo Luini's Applet for Electromagnetic Plane Wave Propagation a model of the penetration & absorption of specific frequency channels for a particular body part. In this instance is a 2.4 GHz wave angling thru the previous example eye's layers @ 30º @ 100% FCC MPE power level of 1mW/cm² using dielectric properties of the typical eye layers from the charts below. You may notice how little this low power 2nd hand WiFi signal has been attenuated passing thru the the iris, ocular fluid, and retina of the eye at a typically glancing angle leaving plenty for the brain to absorb for long term damage and/or promote tumor growth as no doubt Senator McCain suffered.
The first part of this video shows smart meter radiation emissions at typical GSM frequencies of 902-927.5 MHz @ 0.6mW/M², while the second part shows smart meter HAN emissions thru the 2.4GHz WiFi band 2.405-2.430 GHz @ 1.0mW/M² both models do not work concurrently showing that SAR modeling does not often deal with additive effects of multiple transmitters and antennas unlike MPE modeling does.
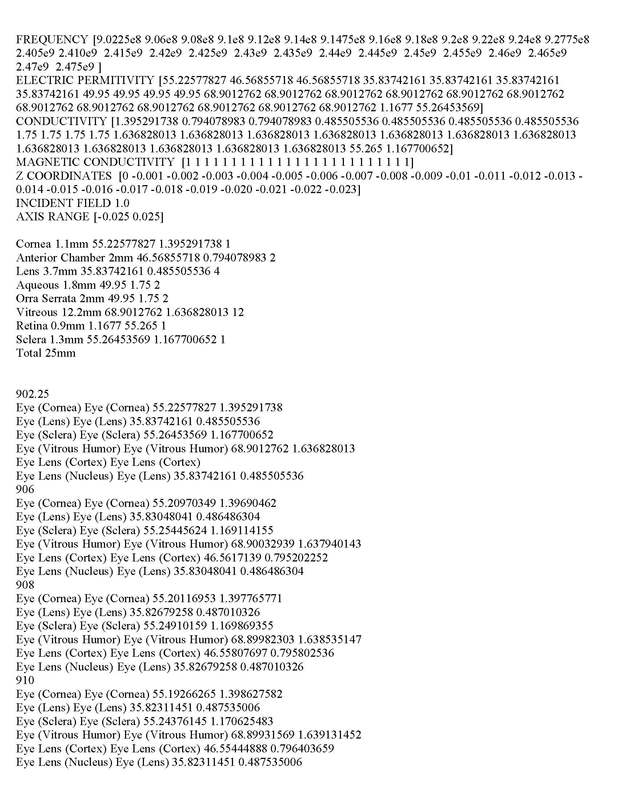
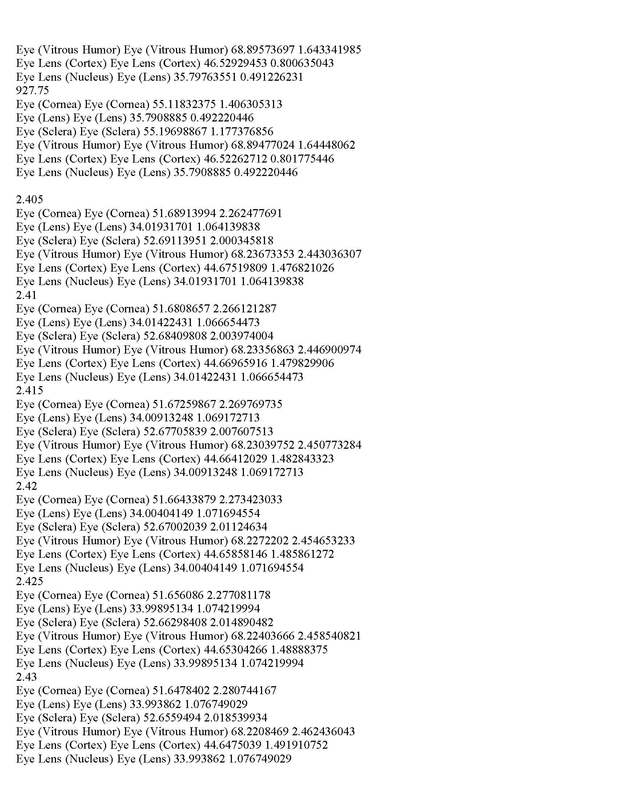
Below is MatLab 2014b modeling sequence calculations with Lorenzo Luini's Applet's 3-D coding inputs which I coded with the above dielectric properties layer/depth/tissue appropriately (note there are actually 2 radio signals in this portable smart meter device a 900 MHz GSM one with 40% lower MPE standards but only one can be modeled with this program at a time).
List of 155 Reviews on Non-thermal Effects of Microwave/Intermediate Frequency EMFs by Martin L. Pall
Among the scientific reviews documenting these various non-thermal health effects are 155 that follow. Each of these reviews cites at least a dozen primary literature citations showing non-thermal effects, with many citing 100 or more going up to the 3rd reference which cites over 1000 such citations. It can be seen from this that the primary literature citations supporting the existence of various non-thermal health effects cited in these reviews go into several thousands. This list is not and is not intended to be a list of all important such reviews. However it gives some measure of the size of the literature that contradicts the industry contention that there are no non-thermal effects of microwave frequency EMFs.
1) Osipov YuA, 1965 [Labor hygiene and the effect of radiofrequency electromagnetic fields on workers]. Leningrad Meditsina Publishing House, 220 pp. 2) Pollack H, Healer J. 1967 Review of Information on Hazards to Personnel from HighFrequency Electromagnetic Radiation. Institute for Defense Analyses; Research and Engineering Support Division. IDA/HQ 67-6211, Series B, May 1967. 3) Naval Medical Research Institute Research Report, June 1971. Bibliography of Reported Biological Phenomena (“Effects”) and Clinical Manifestations, Revised, ZR Glaser. 4) Frey AH. 1971 Biological Function as influenced by low power modulated RF energy. IEEE Trans Microw Theory Tech 19(2): 153-164. 5) Tolgskaya MS, Gordon ZV. 1973. Pathological Effects of Radio Waves, Translated from Russian by B Haigh. Consultants Bureau, New York/London, 146 pages. 6) WHO Document. 1974 Biologic Effects & Health Hazards of Microwave Radiation: Proceedings of an International Symposium, Warsaw, 15-18 October, 1973. http://mistic.heig-vd.ch/taillard/microwave_effects/ 7) Dumanskij, J. D., and Shandala, M. G., 1974. The biologic action and hygienic significance of electromagnetic fields of super-high and ultrahigh frequencies in densely populated areas. Effects and Health Hazards of Microwave Radiation, Proceedings of an International Symposium, Warsaw, 15-18 Oct. 1973, P. Czerski et al., eds. 8) Dwyer, M. J., Leeper, D. B. 1978 A Current Literature Report on the Carcinogenic Properties of Ionizing and Nonionizing Radiation. DHEW Publication (NIOSH) 78-134, March 1978. 9) Bise W. 1978 Low power radio-frequency and microwave effects on human electroencephalogram and behavior. Physiol Chem Phys 10:387-398. 10) Lerner, E. J. 1980. RF radiation: Biological effects. IEEE Spectrum 17(Dec 1980), 51-59. 11) Leach WL. 1980 Genetic, growth and reproductive effects of microwave radiation. Bull N Y Acad Med 56:249-257. 12) Cook HJ, Steneck NH, Vander AJ, Kane GL. 1980 Early research on the biological effects of microwave radiation: 1940-1960. Ann Science 37:323-351. http://discovery.ucl.ac.uk/2223/1/2223.pdf 13) Adey W. R. 1981 Tissue interactions with nonionizing electromagnetic fields. Physiol. Rev. 61, 435-514. 14) Raines, J. K. 1981. Electromagnetic Field Interactions with the Human Body: Observed Effects and Theories. Greenbelt, Maryland: National Aeronautics and Space Administration 1981; 116 p. 15) Marino AA, Morris DH. 1985 Chronic electromagnetic stressors in the environment. A risk factor in human cancer. J environ sci health C3:189-219. 16) Adey WR. 1988 Cell membranes: the electromagnetic environment and cancer promotion. Neurochem Res.13:671-677. 7) Adey WR. 1990 Joint actions of environmental nonionizing electromagnetic fields and chemical pollution in cancer promotion. Environ Health Perspect 86:297-305. 18) Walleczek, J. 1992. Electromagnetic field effects on cells of the immune system: the role of calcium signaling. FASEB J. 6, 3177-3185. 19) Adey, WR. 1993 Biological effects of electromagnetic fields. J Cell Biochem 51:410-416. 20) Bolen, S. M. 1994 Radiofrequency/Microwave Radiation Biological Effects and safety standards: a review. AD-A282 886, Rome Laboratory, U.S. Air Force Material Command, Griffiss Air Force Base, New York. 21) Lai H. 1994 Neurological effects of radiofrequency electromagnetic radiation. In: Advances in Electromagnetic Fields in Living Systems, Vol. 1, J.C. Lin, Ed., Plenum Press, New York, pp. 27-88. 22) Goldsmith JR. 1995 Epidemiological evidence of radiofrequency radiation (microwave) effects on health in military, broadcasting and occupational settings. Int J Occup Environ Health 1:47-57. 23) Goodman EM, Greenebaum B, Marron MT. 1995 Effects of electromagnetic fields on molecules and cells. Int Rev Cytol 158:279-338. 24) Grigoriev IUG. 1996 Role of modulation in biological effects of electromagnetic radiation. Radiats Biol Radioecol 36:659-670. 25) Lai, H. 1997. Neurological effects of radiofrequency electromagnetic radiation relating to wireless communication technology. Paper presented at the IBC-UK Conference: “Mobile Phones – Is There a Health Risk?” http://www.mapcruzin.com/radiofrequency/henry_lai1.htm 26) Adey WR, 1997 Bioeffects of mobile communications fields: possible mechanisms for cumulative dose. In: N Kuster, Q Balzano, JC Lin (Eds), Mobile Communications Safety, New York, Chapman and Hall, pp. 95-131. 27) Goldsmith JR. 1997 Epidemiologic evidence relevant to radar (microwave) effects. Env Health Perspect 105(Suppl 6):1579-1587. 28) Frey, A. H. 1998. Headaches from cellular telephones: are they real and what are the implications? Environ. Health Perspect. 106, 101-103. 29) Lai, H 1998 Neurological effects of radiofrequency electromagnetic radiation. http://www.mapcruzin.com/radiofrequency/henry_lai2.htm. 30) Hyland GJ. 1998 Non-thermal bioeffects induced by low-intensity microwave frequency microwave irradiation of living systems. Engineering Science Educ J 7(6):261-269. 31) Ryabi JT. 1998 Clinical effects of electromagnetic fields on fracture healing. Clin Orthop Relat Res 355(Suppl. l): S205–15. 32) Barnett SB. 1999 Radio-frequency radiation and birth defects: Is there a threat to human health? Cong Anom 39:59-73. 33) Belyaev IY, Shcheglov VS, Alipov ED, Ushakov VD. 2000 Nonthermal Effects of Extremely High-Frequency Microwaves on Chromatin Conformation in Cells in vitro—Dependence on Physical, Physiological, and Genetic Factors. IEEE Trans Microwave Theory Tech 48:21722179. 34) Betskii OV, Devyatkov ND, Kislov VV. 2000 Low intensity millimeter waves in medicine and biology. Crit Rev Biomed Eng. 2000;28(1-2):247-268. 35) Somosy Z. 2000 Radiation response of cell organelles. Micron 31:165-181 36) Krewski D, Byus CV, Glickman BW, Lotz WG, Mandeville R, McBride ML, Prato FS, Weaver DF. 2001 Potential health risks of radiofrequency fields from wireless telecommunication devices. J Toxicol Environ Health B Crit Rev 4: 1-143. 37) Banik S, Bandyopadhyay S, Ganguly S. 2003 Bioeffects of microwave--a brief review. Bioresour Technol. 2003 Apr;87(2):155-9. 38) Blank M, Goodman R. 2004 Comment: a biological guide for electromagnetic safety : the stress response. Bioelectromagnetics 25(8):642-646. 39) Kundi M, Kild K, Hardell L, Mattsson M. 2004 Mobile telephones and cancer – a review of the epidemiological evidence. J Toxicol Env Health, Part B 7:351-384. 40) Karasek M, Woldanska-Okonska M. 2004 Electromagnetic fields and human endocrine system. ScientificWorldJournal. 2004 Oct 20;4 Suppl 2:23-28. 41) Kundi M. 2004 Mobile phone use and cancer. Occup Env Med 61:560-570. 42) Aaron RK, Ciombor DM, Simon BJ. 2004 Treatment of nonunions with electric and electromagnetic fields. Clin Orthop Relat Res 2004; 10: 579–593. 43) Belyaev I. 2005 Non-thermal biological effects of microwaves: current knowledge, further perspective and urgent needs. Electromagn Biol Med 24(3):375-403. 44) Belyaev I. 2005 Non-thermal biological effects of microwaves. Microwave Rev 11(2):13-29. 45) Barnes FS, Greenebaum B, (eds.) 2007 Biological and medical aspects of electromagnetic fields. 3rd, ed., CRC Press, Boca Raton, FL. 46) Behari J, Paulraj R. 2007 Biomarkers of induced electromagnetic field and cancer. Indian J Exp Biol 45:77-85. 47) Bioinitiative Working Group, Cindy Sage and David Carpenter (eds). 2007 Bioinitiative report: A rationale for a biologically-based public exposure standard for electromagnetic fields (ELF and RF). www.bioinitiative.org 48) Huss A, Egger M, Hug K, Huwiler-Müntener K, Röösli M. 2007 Source of funding and results of studies of health effects of mobile phone use: systematic review of experimental studies. Environ Health Perspect 115:1–4. 49) Markov MS. 2007 Pulsed electromagnetic field therapy: History, state of the art and future. The Environmentalist 27:465-475. 50) Nittby H, Grafstrom G, Eberhardt JL, Malmgren L, Brun A, Persson BR, Salford, LG. 2008 Radiofrequency and extremely low frequency electromagnetic field effects on the bloodbrain barrier. Electromag Biol Med 2008; 27:103-126. 51) Hazout A, Menezo Y, Madelenat P, Yazbeck C, Selva J, Cohen-Bacrie P. 2008 [Causes and clinical implications of sperm DNA damages]. [Article in French] Gynecol Obstet Fertil 36:1109-1117. 52) Hardell, L., Sage, C. 2008. Biological effects from electromagnetic field exposure and public exposure standards. Biomed. Pharmacother. 62, 104-109. 53) Genuis SJ. 2008 Fielding a current idea: exploring the public health impact of electromagnetic radiation. Public Health 122:113-124. 54) Johansson O. 2009 Disturbance of the immune system by electromagnetic fields-A potentially underlying cause for cellular damage and tissue repair reduction which could lead to disease and impairment. Pathophysiology 16:157-177. 55) Blackman C. 2009 Cell phone radiation: Evidence from ELF and RF studies supporting more inclusive risk identification and assessment. Pathophysiology. 2009 Aug;16(2-3):205-216 56) Balmori A. 2009 Electromagnetic pollution from phone masts. Effects on wildlife. Pathophysiology 16:191-199. 57) Davanipour Z, Sobel E. 2009 Long-term exposure to magnetic fields and the risks of Alzheimer's disease and breast cancer: Further biological research. Pathophysiology 16:149-156. 58) Desai NR, Kesari KK, Agarwal A. 2009 Pathophysiology of cell phone radiation: oxidative stress and carcinogenesis with focus on the male reproductive system. Reproduct Biol Endocrinol 7:114. 59) Khurana VG, Teo C, Kundi M, Hardell L, Carlberg M. 2009 Cell phones and brain tumors: a review including the long-term epidemiologic data. Surg Neurol 72:205-214. 60) Martin Blank, Reba Goodman. 2009 Electromagnetic fields stress living cells. Pathophysiology 16:71-78. 61) Phillips JL, Singh NP, Lai H. 2009 Electromagnetic fields and DNA damage. Pathophysiology 16:79-88. 62) Makker K, Varghese A, Desai NR, Mouradi R, Agarwal A. 2009 Cell phones: modern man's nemesis? Reprod Biomed Online 18:148-157. 63) Ruediger HW. 2009 Genotoxic effects of radiofrequency electromagnetic fields. Pathophysiology. 16:89-102. 64) Yakymenko I, Sidorik E. 2010 Risks of carcinogenesis from electromagnetic radiation and mobile telephony devices. Exp Oncol 32:729-736. 65) Carpenter DO. 2010 Electromagnetic fields and cancer: the cost of doing nothing. Rev Environ Health 25:75-80. 66) Khurana, V. G., Hardell, L., Everaert, J., Bortkiewicz, A., Carlberg, M., Ahonen, M. 2010 Epidemiological evidence for a health risk from mobile phone base stations. Int. J. Occup. Environ. Health 16, 263-267. 67) Giuliani L, Soffriti M (Eds). 2010 NON-THERMAL EFFECTS AND MECHANISMS OF INTERACTION BETWEEN ELECTROMAGNETIC FIELDS AND LIVING MATTER, RAMAZZINI INSTITUTE EUR. J. ONCOL. LIBRARY Volume 5, National Institute for the Study and Control of Cancer and Environmental Diseases “Bernardino Ramazzini” Bologna, Italy 2010, 400 page monograph. 68) Fragopoulou A, Grigoriev Y, Johansson O, Margaritis LH, Morgan L, Richter E, Sage C. Scientific panel on electromagnetic field health risks: consensus points, recommendations, and rationales. Rev. Environ. Health 25, 307-317. 69) Batista Napotnik T, Reberšek M, Vernier PT, Mali B, Miklavčič D. 2010 Effects of high voltage nanosecond electric pulses on eukaryotic cells (in vitro): A systematic review. Bioelectrochemistry 110:1-12. 70) Levitt, B. B., Lai, H. 2010. Biological effects from exposure to electromagnetic radiation emitted by cell tower base stations and other antenna arrays. Environ. Rev. 18, 369-395. 71) Yu Y, Yao K. 2010 Non-thermal cellular effects of low power microwave radiation on the lens and lens epithelial cells. J Int Med Res 38:729-736. 72) Yakymenko, I., Sidorik, E., Kyrylenko, S., Chekhun, V. 2011. Long-term exposure to microwave radiation provokes cancer growth: evidences from radars and mobile communication systems. Exp. Oncol. 33(2), 62-70. 73) Kesari KK, Kuman S, Behari J. 2011 Effects of radiofrequency electromagnetic wave exposure from cellular phones on reproductive pattern in male Wistar rats. Appl Biochem Biotechnol 164:546-549. 74) Panagopoulos DJ. 2011 Analyzing the health impacts of modern telecommunication microwaves. Chapter 1 in Advances in Biology and Medicine, Vol. 17, Leon V. Berhardt, Ed., Nova Science Publishers. 75) Schidt-Rohlfing B, Silny J, Gavenis K, et al. 2011 Electromagnetic fields, electric current and bone healing – what is the evidence? Z Orthop Unfall. 149: 265–270. 76) Chalidis B, Sachinis N, Assiotis A, et al. 2011 Stimulation of bone formation and fracture healing with pulsed electromagnetic fields: biologic responses and clinical implica- tions. Int J Immunopathol Pharmacol. 2011; 24(1 Suppl. 2): 17020. 77) Pilla A, Fitzsimmons R, Muehsam D, et al. 2011 Electromagnetic fields as first messenger in biological signaling: application to calmodulin-dependent signaling in tissue repair. Biochim Biophys Acta 1810: 1236–1245. 78) Yakimenko IL, Sidorik EP, Tsybulin AS. 2011 [Metabolic changes in cells under electromagnetic radiation of mobile communication systems]. [Article in Russian] Ukr Biokhim Zh 83:20-28. 79) La Vignera, Condorelli RA, Vicari E, D’Agata R, Calogero AE. 2012 Effects of the exposure to mobile phones on male reproduction: a review of the literature. J Androl 33:350-356. 80) Zhong C, Zhao TF, Xu ZJ, et al. 2012 Effects of electromagnetic fields on bone regeneration in experimental and clinical studies: a review of the literature. Chin Med J 125: 367–372. 81) Biointiative Working Group, David Carpenter and Cindy Sage (eds). 2012 Bioinitiative 2012: A rationale for biologically-based exposure standards for electromagnetic radiation. http://www.bioinitiative.org/participants/why-we-care/ 82) Gye MC, Park CJ. 2012 Effect of electromagnetic field exposure on the reproductive system. Clin Exp Reprod Med 39:1-9. 83) Trošić I, Pavičić I, Marjanović AM, Bušljeta I. 2012 Non-thermal biomarkers of exposure to radiofrequency/microwave radiation. Arh Hig Rada Toksikol 63 Suppl 1:67-73. 84) Consales, C., Merla, C., Marino, C., et al. 2012. Electromagnetic fields, oxidative stress, and neurodegeneration. Int. J. Cell Biol. 2012: 683897. 85) Havas, M. 2013. Radiation from wireless technology affects the blood, the heart, and the autonomic nervous system. Rev. Environ. Health. 28(Nov 2013), 75-84. 86) Herbert, M. R., Sage, C. 2013 Autism and EMF? Plausibility of a pathophysiological link – Part I. Pathophysiology 20, 191-209. 87) Herbert, M. R., Sage, C. 2013. Autism and EMF? Plausibility of a pathophysiological link part II. Pathophysiology 20, 211-234. 88) Jayasanka SMDH, Asaeda T. 2013 The significance of microwaves in the environment and its effects on plants. Envron Rev 22:220-228. 89) Kesari KK, Siddiqui MH, Meena R, Verma HN, Kumar S. 2013 Cell phone radiation exposure on brain and associated biological systems. Indian J Exp Biol 51:187-200. 90) Warnke U, Hensinger P. 2013 Increasing incidence of burnout due to magnetic fields of cell phone networks and other wireless communication technologies. Umwelt Medizin Gesellshaft 26: 31-38. 91) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2013. Evaluation of specific absorption rate as a dosimetric quantity for electromagnetic fields bioeffects. PloS ONE 8(6): e62663. doi:10:1371 92) Carpenter DO. 2013. Human disease resulting from exposure to electromagnetic fields. Rev Environ Health. 2013;28(4):159-72. 93) Ledoigt G, Belpomme D. 2013 Cancer induction molecular pathways and HF-EMF irradiation. Adv Biol Chem 3:177-186. 94) Pall, ML. 2013. Electromagnetic fields act via activation of voltage-gated calcium channels to produce beneficial or adverse effects. J. Cell. Mol. Med. 17:958-965. 95) Pilla, AA. 2013 Nonthermal electromagnetic fields: from first messenger to therapeutic applications. Electromagn. Biol. Med. 32, 123-136. 96) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2013. Evaluation of specific absorption rate as a dosimetric quantity for electromagnetic fields bioeffects. PloS ONE 8(6): e62663. doi:10:1371 97) Halgamuge MN. 2013 Pineal melatonin level disruption in humans due to electromagnetic fields and ICNIRP limits. Radiat Prot Dosimetr 154: 405-416 98) Szmigielski S. 2013 Reaction of the immune system to low-level RF/MW exposures. Sci Total Environ 2013 Jun 1;454-455:393-400. 99) Hardell L, Carlberg M, Hansson Mild K. 2013 Use of mobile phones and cordless phones is associated with increased risk for glioma and acoustic neuroma. Pathophysiology 2013;20(2):85-110. 100) Davis DL, Kesari S, Soskolne CL, Miller AB, Stein Y. 2013 Swedish review strengthens grounds for concluding that radiation from cellular and cordless phones is a probable human carcinogen. Pathophysiology 20:123-129. 101) Naziroglu M, Yuksel M, Kose SA, Ozkaya MO. 2013 Recent reports of Wi-Fi and mobile phone-induced radiation on oxidative stress and reproductive signaling pathways in females and males. [review] J Membr Biol 246 (12): 869-875. 102) Adams, J. A., Galloway, T. S., Mondal, D., Esteves, S. C. 2014 Effect of mobile telephones on sperm quality: A systematic review and meta-analysis. Environment. Int. 70, 106-112. 103) Murbach, M., Neufeld, E., Christopoulou, M., Achermann, P., Kuster, N. 2014. Modeling of EEG electrode artifacts and thermal ripples in human radiofrequency exposure studies. Bioelectromagnetics 35, 273-283. 104) Lewczuk B, Redlarski G, Zak A, Ziółkowska N, Przybylska-Gornowicz B, Krawczuk M. 2014 Influence of electric, magnetic, and electromagnetic fields on the circadian system: current stage of knowledge. Biomed Res Int. 2014;2014:169459. doi: 10.1155/2014/169459. Epub 2014 Jul 22. 105) Van Boxem K, Huntoon M, Van Zundert J, Patijn J, van Kleef M, Joosten EA. 2014 Pulsed radiofrequency: a review of the basic science as applied to the pathophysiology of radicular pain: a call for clinical translation. Reg Anesth Pain Med. 2014 Mar-Apr;39(2):14959. 106) Liu K, Li Y, Zhang G, Liu J, Cao J, Ao L, Zhang S. 2014 Association between mobile phone use and semen quality: a systematic review and meta-analysis. Andrology 2:491-501. 107) Pilla, AA 2015 Pulsed electromagnetic fields: from signaling to healing. In: Markov, M. S., Ed. 2015. Electromagnetic Fields in Biology and Medicine. CRC Press, Taylor and Francis Group, Boca Raton, FL. , pp. 29-40.108) Belyaev, I. 2015. Biophysical mechanisms for nonthermal microwave effects. In: Electromagnetic Fields in Biology and Medicine, Marko S. Markov, ed, CRC Press, New York, pp 49-67. (Please note: There are probably a dozen other reviews that from this volume that might be included here on non-thermal effects) 109) Sangün Ö, Dündar B, Çömlekçi S, Büyükgebiz A. 2015 The Effects of Electromagnetic Field on the Endocrine System in Children and Adolescents. Pediatr Endocrinol Rev 13:531-545. 110) Pall, M. L. 2015. Scientific evidence contradicts findings and assumptions of Canadian Safety Panel 6: microwaves act through voltage-gated calcium channel activation to induce biological impacts at non-thermal levels, supporting a paradigm shift for microwave/lower frequency electromagnetic field action. Rev. Environ. Health 3, 99-116. 111) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2015. Real versus simulated mobile phone exposures in experimental studies. BioMed. Res. Int. 2015, article ID 607053, 8 pages. 112) Mahdavi M, Yekta R, Tackallou SH. 2015 Positive correlation between ELF and RF electromagnetic fields on cancer risk. J Paramed Sci 6(3), ISSN 2008-4978. 113) Morgan LL, Miller AB, Sasco A, Davis DL. 2015 Mobile phone radiation causes brain tumors and should be classified as a probable human carcinogen (2A). Int J Oncol 46(5): 1865-71. 114) Vadalà M, Vallelunga A, Palmieri L, Palmieri B, Morales-Medina JC, Iannitti T. 2015 Mechanisms and therapeutic applications of electromagnetic therapy in Parkinson's disease. Behav Brain Funct. 2015 Sep 7;11:26. doi: 10.1186/s12993-015-0070-z. 115) Lim R, Lee SW, Tan PY, Liong ML, Yuen KH. 2015 Efficacy of electromagnetic therapy for urinary incontinence: A systematic review. Neurourol Urodyn 34(8):713-722. 116) Hedendahl L, Carlberg M, Hardell L. 2015 Electromagnetic hypersensitivity – an increasing challenge to the medical profession. Rev Environ Health 30:209-215. 117) Carpenter DO. 2015 The microwave syndrome or electro-hypersensitivity: historical background. Rev Environ Health. 30:217-222. 118) Yakymenko I, Tsybulin O, Sidorik E, Henshel D, Kyrylenko O, Kysylenko S. 2015 Oxidative mechanisms of biological activity of low-intensity radiofrequency radiation. Electromagnetic Biol Med: Early Online 1-16. ISSN: 1536-8378. 119) Panagopoulos DJ, Johansson O, Carlo GL. 2015 Polarization: A Key Difference between Man-made and Natural Electromagnetic Fields, in regard to Biological Activity. Sci Rep. 2015 Oct 12;5:14914. doi: 10.1038/srep14914. 120) Sage C. 2015 The implications of non-linear biological oscillations on human electrophysiology for electrohypersensitivity (EHS) and multiple chemical sensitivity (MCS). Rev Environ Health. 2015;30(4):293-303. 121) Eghlidospour M, Mortazavi SM, Yousefi F, Mortazavi SA. 2015 New Horizons in Enhancing the Proliferation and Differentiation of Neural Stem Cells Using Stimulatory Effects of the Short Time Exposure to Radiofrequency Radiation. J Biomed Phys Eng. 2015 Sep 1;5(3):95-104. eCollection 2015 Sep. 122) Kaszuba-Zwoińska J, Gremba J, Gałdzińska-Calik B, Wójcik-Piotrowicz K, Thor PJ. 2015 Electromagnetic field induced biological effects in humans. Przegl Lek. 2015;72(11):636-41. 123) K Sri N. 2015 Mobile Phone Radiation: Physiological & Pathophysiologcal Considerations. Indian J Physiol Pharmacol. 2015 Apr-Jun;59(2):125-35. 124) Redmayne M, Johansson O. 2015 Radiofrequency exposure in young and old: different sensitivities in light of age-relevant natural differences. Rev Environ Health 30: 323-335. 125) Pall, ML. 2016. Microwave frequency electromagnetic fields (EMFs) produce widespread neuropsychiatric effects including depression. J. Chem. Neuroanat. 75(Pt B):4351. 126) Warille AA, Onger ME, Turkmen AP, Deniz ÖG, Altun G, Yurt KK, Altunkaynak BZ, Kaplan S. 2016 Controversies on electromagnetic field exposure and the nervous systems of children. Histol Histopathol 31(5):461-468.27) Vian A, Davies E, Gendraud M, Bonnet P. 2016 Plant Responses to High Frequency Electromagnetic Fields. Biomed Res Int. 2016;2016:1830262. doi: 10.1155/2016/1830262. Epub 2016 Feb 14. 128) Kaplan S, Deniz OG, Önger ME, Türkmen AP, Yurt KK, Aydın I, Altunkaynak BZ, Davis D. 2016 Electromagnetic field and brain development. J Chem Neuroanat 75(Pt B):52-61. 129) Altunkaynak BZ, Altun G, Yahyazadeh A, Kaplan AA, Deniz OG, Türkmen AP, Önger ME, Kaplan S. 2016 Different methods for evaluating the effects of microwave radiation exposure on the nervous system. J Chem Neuroanat. 2016 Sep;75(Pt B):62-9. 130) Dasdag S, Akdag MZ. 2016 The link between radiofrequencies emitted from wireless technologies and oxidative stress. J Chem Neuroanat. 2016 Sep;75(Pt B):85-93. 131) Terzi M, Osberk B, Deniz OG, Kaplan S. 2016 The role of electromagnetic fields in neurological disorders. . J Chem Neuroanat. 2016 Sep;75(Pt B):77-84. 132) Maziarz A, Kocan B, Bester M, Budzik S, Cholewa M, Ochiya T, Banas A. 2016 How electromagnetic fields can influence adult stem cells: positive and negative impacts. Stem Cell Res Ther 2016 Apr 18;7(1):54. doi: 10.1186/s13287-016-0312-5. 133) Soghomonyan D, Trchounian K, Trchounian A. 2016 Millimeter waves or extremely high frequency electromagnetic fields in the environment: what are their effects on bacteria? Appl Microbiol Biotechnol. 100:4761-4771. 134) Maes A, Verschaeve L. 2016 Genetic damage in humans exposed to extremely lowfrequency electromagnetic fields. Arch Toxicol. 2016 Jun 23. [Epub ahead of print] 135) Belyaev I, Dean A, Eger H, Hubmann G, Jandrisovits R, Johansson O, Kern M, Kundi M, Lercher P, Mosgöller W, Moshammer H, Müller K, Oberfeld G, Ohnsorge P, Pelzmann P, Scheingraber C, Thill R. 2016 EUROPAEM EMF Guideline 2016 for the prevention, diagnosis and treatment of EMF-related health problems and illnesses. Rev. Environ. Health DOI 10.1515/reveh-2016-0011. 136) Pall ML. 2016 Electromagnetic fields act similarly in plants as in animals: Probable activation of calcium channels via their voltage sensor. Curr Chem Biol 10:74-82. 137) Medeiros LN, Sanchez TG. 2016 Tinnitus and cell phones: the role of electromagnetic radiofrequency radiation. Braz J Otorhinolaryngol. 2016 Jan-Feb;82(1):97104. 138) Starkey SJ. 2016 Inaccurate official assessment of radiofrequency safety by the Advisory Group on Non-ionising Radiation. Rev Environ Health 31:493-503. 139) Hecht K. 2016 Health Implications of Long-term Exposure to Electrosmog: Effects of Wireless Communication Technologies, pp 1-64. Brochure 6 of A Brochure Series of the Competence Initiative for the Protection of Humanity, the Environment and Democracy E.V. URL: http://kompetenzinitiative.net/KIT/wp-content/uploads/2016/07/KI_Brochure6_K_Hecht_web.pdf 140) Asghari A, Khaki AA, Rajabzadeh A, Khaki A. 2016 A review on electromagnetic fields (EMFs) and the reproductive system. Electron Physician. 2016 Jul 25;8(7):2655-62. 141) Houston BJ, Nixon B, King BV, De Iuliis GN, Aitken RJ. 2016 The effects of radiofrequency electromagnetic radiation on sperm function. Reproduction. 2016 Dec;152(6):R263-R276. 142) Halgamuge MN. 2017 Review: Weak radiofrequency radiation exposure from mobile phone radiation on plants. Electromagn Biol Med. 2017;36(2):213-235. 143) Bortkiewicz A, Gadzicka E, Szymczak W. 2017 Mobile phone use and risk for intracranial tumors and salivary gland tumors - A meta-analysis. Int J Occup Med Environ Health. 2017 Feb 21;30(1):27-43. 144) Carlberg M, Hardell L. 2017 Evaluation of Mobile Phone and Cordless Phone Use and Glioma Risk Using the Bradford Hill Viewpoints from 1965 on Association or Causation. BioMed Res Int 2017, Article ID 9218486, https://doi.org/10.1155/2017/9218486 145) Bielsa-Fernández P, Rodríguez-Martín B. 2017 [Association between radiation from mobile phones and tumour risk in adults]. Gac Sanit. 2017 Apr 12. pii: S02139111(17)30083-3. doi: 10.1016/j.gaceta.2016.10.014. [Epub ahead of print] 146) Alegría-Loyola MA, Galnares-Olalde JA, Mercado M. 2017 [Tumors of the central nervous system]. Rev Med Inst Mex Seguro Soc. 2017 May-Jun;55(3):330-340. 47) Miah T, Kamat D. 2017 Current Understanding of the Health Effects of Electromagnetic Fields. Pediatr Ann. 2017 Apr 1;46(4):e172-e174. doi: 10.3928/1938235920170316-01. 148) Facchini G, Spinnato P, Guglielmi G, Albisinni U, Bazzocchi A. 2017 A comprehensive review of pulsed radiofrequency in the treatment of pain associated with different spinal conditions. Br J Radiol. 2017 May;90(1073):20150406. doi: 10.1259/bjr.20150406. Epub 2017 Feb 10. 149) Kim K, Jo D, Kim E. 2017 Pulsed Radiofrequency to the Dorsal Root Ganglion in Acute Herpes Zoster and Postherpetic Neuralgia. Pain Physician. 2017 Mar;20(3):E411E418. 150) Prasad M, Kathuria P, Nair P, Kumar A, Prasad K. 2017 Mobile phone use and risk of brain tumours: a systematic review of association between study quality, source of funding, and research outcomes. Neurol Sci. 2017 Feb 17. doi: 10.1007/s10072-017-2850-8. [Epub ahead of print]. 151) Bandara P, Weller S. 2017 Cardiovascular disease: Time to identify emerging environmental factors. Eur J Prevent Cardiol 24(17):1819-1823. 152) Wang J, Su H, Xie W, Yu S. Mobile Phone Use and The Risk of Headache: A Systematic Review and Meta-analysis of Cross-sectional Studies. Sci Rep. 2017 Oct 3;7(1):12595. doi: 10.1038/s41598-017-12802-9. 153) .Mishra SK, Chowdhary R, Kumari S, Rao SB. 2017 Effect of Cell Phone Radiations on Orofacial Structures: A Systematic Review. J Clin Diagn Res. 2017 May;11(5):ZE01-ZE05. doi: 10.7860/JCDR/2017/26547.9883. Epub 2017 May 1 154) Hardell L. 2017 World Health Organization, radiofrequency radiation and health – a hard nut to crack (Review). Int J Oncol 51:405-413. 155) Wang H, Zhang X. 2017 Magnetic Fields and Reactive Oxygen Species. Int J Mol Sci. 2017 Oct 18;18(10). pii: E2175. doi: 10.3390/ijms18102175.
Among the scientific reviews documenting these various non-thermal health effects are 155 that follow. Each of these reviews cites at least a dozen primary literature citations showing non-thermal effects, with many citing 100 or more going up to the 3rd reference which cites over 1000 such citations. It can be seen from this that the primary literature citations supporting the existence of various non-thermal health effects cited in these reviews go into several thousands. This list is not and is not intended to be a list of all important such reviews. However it gives some measure of the size of the literature that contradicts the industry contention that there are no non-thermal effects of microwave frequency EMFs.
1) Osipov YuA, 1965 [Labor hygiene and the effect of radiofrequency electromagnetic fields on workers]. Leningrad Meditsina Publishing House, 220 pp. 2) Pollack H, Healer J. 1967 Review of Information on Hazards to Personnel from HighFrequency Electromagnetic Radiation. Institute for Defense Analyses; Research and Engineering Support Division. IDA/HQ 67-6211, Series B, May 1967. 3) Naval Medical Research Institute Research Report, June 1971. Bibliography of Reported Biological Phenomena (“Effects”) and Clinical Manifestations, Revised, ZR Glaser. 4) Frey AH. 1971 Biological Function as influenced by low power modulated RF energy. IEEE Trans Microw Theory Tech 19(2): 153-164. 5) Tolgskaya MS, Gordon ZV. 1973. Pathological Effects of Radio Waves, Translated from Russian by B Haigh. Consultants Bureau, New York/London, 146 pages. 6) WHO Document. 1974 Biologic Effects & Health Hazards of Microwave Radiation: Proceedings of an International Symposium, Warsaw, 15-18 October, 1973. http://mistic.heig-vd.ch/taillard/microwave_effects/ 7) Dumanskij, J. D., and Shandala, M. G., 1974. The biologic action and hygienic significance of electromagnetic fields of super-high and ultrahigh frequencies in densely populated areas. Effects and Health Hazards of Microwave Radiation, Proceedings of an International Symposium, Warsaw, 15-18 Oct. 1973, P. Czerski et al., eds. 8) Dwyer, M. J., Leeper, D. B. 1978 A Current Literature Report on the Carcinogenic Properties of Ionizing and Nonionizing Radiation. DHEW Publication (NIOSH) 78-134, March 1978. 9) Bise W. 1978 Low power radio-frequency and microwave effects on human electroencephalogram and behavior. Physiol Chem Phys 10:387-398. 10) Lerner, E. J. 1980. RF radiation: Biological effects. IEEE Spectrum 17(Dec 1980), 51-59. 11) Leach WL. 1980 Genetic, growth and reproductive effects of microwave radiation. Bull N Y Acad Med 56:249-257. 12) Cook HJ, Steneck NH, Vander AJ, Kane GL. 1980 Early research on the biological effects of microwave radiation: 1940-1960. Ann Science 37:323-351. http://discovery.ucl.ac.uk/2223/1/2223.pdf 13) Adey W. R. 1981 Tissue interactions with nonionizing electromagnetic fields. Physiol. Rev. 61, 435-514. 14) Raines, J. K. 1981. Electromagnetic Field Interactions with the Human Body: Observed Effects and Theories. Greenbelt, Maryland: National Aeronautics and Space Administration 1981; 116 p. 15) Marino AA, Morris DH. 1985 Chronic electromagnetic stressors in the environment. A risk factor in human cancer. J environ sci health C3:189-219. 16) Adey WR. 1988 Cell membranes: the electromagnetic environment and cancer promotion. Neurochem Res.13:671-677. 7) Adey WR. 1990 Joint actions of environmental nonionizing electromagnetic fields and chemical pollution in cancer promotion. Environ Health Perspect 86:297-305. 18) Walleczek, J. 1992. Electromagnetic field effects on cells of the immune system: the role of calcium signaling. FASEB J. 6, 3177-3185. 19) Adey, WR. 1993 Biological effects of electromagnetic fields. J Cell Biochem 51:410-416. 20) Bolen, S. M. 1994 Radiofrequency/Microwave Radiation Biological Effects and safety standards: a review. AD-A282 886, Rome Laboratory, U.S. Air Force Material Command, Griffiss Air Force Base, New York. 21) Lai H. 1994 Neurological effects of radiofrequency electromagnetic radiation. In: Advances in Electromagnetic Fields in Living Systems, Vol. 1, J.C. Lin, Ed., Plenum Press, New York, pp. 27-88. 22) Goldsmith JR. 1995 Epidemiological evidence of radiofrequency radiation (microwave) effects on health in military, broadcasting and occupational settings. Int J Occup Environ Health 1:47-57. 23) Goodman EM, Greenebaum B, Marron MT. 1995 Effects of electromagnetic fields on molecules and cells. Int Rev Cytol 158:279-338. 24) Grigoriev IUG. 1996 Role of modulation in biological effects of electromagnetic radiation. Radiats Biol Radioecol 36:659-670. 25) Lai, H. 1997. Neurological effects of radiofrequency electromagnetic radiation relating to wireless communication technology. Paper presented at the IBC-UK Conference: “Mobile Phones – Is There a Health Risk?” http://www.mapcruzin.com/radiofrequency/henry_lai1.htm 26) Adey WR, 1997 Bioeffects of mobile communications fields: possible mechanisms for cumulative dose. In: N Kuster, Q Balzano, JC Lin (Eds), Mobile Communications Safety, New York, Chapman and Hall, pp. 95-131. 27) Goldsmith JR. 1997 Epidemiologic evidence relevant to radar (microwave) effects. Env Health Perspect 105(Suppl 6):1579-1587. 28) Frey, A. H. 1998. Headaches from cellular telephones: are they real and what are the implications? Environ. Health Perspect. 106, 101-103. 29) Lai, H 1998 Neurological effects of radiofrequency electromagnetic radiation. http://www.mapcruzin.com/radiofrequency/henry_lai2.htm. 30) Hyland GJ. 1998 Non-thermal bioeffects induced by low-intensity microwave frequency microwave irradiation of living systems. Engineering Science Educ J 7(6):261-269. 31) Ryabi JT. 1998 Clinical effects of electromagnetic fields on fracture healing. Clin Orthop Relat Res 355(Suppl. l): S205–15. 32) Barnett SB. 1999 Radio-frequency radiation and birth defects: Is there a threat to human health? Cong Anom 39:59-73. 33) Belyaev IY, Shcheglov VS, Alipov ED, Ushakov VD. 2000 Nonthermal Effects of Extremely High-Frequency Microwaves on Chromatin Conformation in Cells in vitro—Dependence on Physical, Physiological, and Genetic Factors. IEEE Trans Microwave Theory Tech 48:21722179. 34) Betskii OV, Devyatkov ND, Kislov VV. 2000 Low intensity millimeter waves in medicine and biology. Crit Rev Biomed Eng. 2000;28(1-2):247-268. 35) Somosy Z. 2000 Radiation response of cell organelles. Micron 31:165-181 36) Krewski D, Byus CV, Glickman BW, Lotz WG, Mandeville R, McBride ML, Prato FS, Weaver DF. 2001 Potential health risks of radiofrequency fields from wireless telecommunication devices. J Toxicol Environ Health B Crit Rev 4: 1-143. 37) Banik S, Bandyopadhyay S, Ganguly S. 2003 Bioeffects of microwave--a brief review. Bioresour Technol. 2003 Apr;87(2):155-9. 38) Blank M, Goodman R. 2004 Comment: a biological guide for electromagnetic safety : the stress response. Bioelectromagnetics 25(8):642-646. 39) Kundi M, Kild K, Hardell L, Mattsson M. 2004 Mobile telephones and cancer – a review of the epidemiological evidence. J Toxicol Env Health, Part B 7:351-384. 40) Karasek M, Woldanska-Okonska M. 2004 Electromagnetic fields and human endocrine system. ScientificWorldJournal. 2004 Oct 20;4 Suppl 2:23-28. 41) Kundi M. 2004 Mobile phone use and cancer. Occup Env Med 61:560-570. 42) Aaron RK, Ciombor DM, Simon BJ. 2004 Treatment of nonunions with electric and electromagnetic fields. Clin Orthop Relat Res 2004; 10: 579–593. 43) Belyaev I. 2005 Non-thermal biological effects of microwaves: current knowledge, further perspective and urgent needs. Electromagn Biol Med 24(3):375-403. 44) Belyaev I. 2005 Non-thermal biological effects of microwaves. Microwave Rev 11(2):13-29. 45) Barnes FS, Greenebaum B, (eds.) 2007 Biological and medical aspects of electromagnetic fields. 3rd, ed., CRC Press, Boca Raton, FL. 46) Behari J, Paulraj R. 2007 Biomarkers of induced electromagnetic field and cancer. Indian J Exp Biol 45:77-85. 47) Bioinitiative Working Group, Cindy Sage and David Carpenter (eds). 2007 Bioinitiative report: A rationale for a biologically-based public exposure standard for electromagnetic fields (ELF and RF). www.bioinitiative.org 48) Huss A, Egger M, Hug K, Huwiler-Müntener K, Röösli M. 2007 Source of funding and results of studies of health effects of mobile phone use: systematic review of experimental studies. Environ Health Perspect 115:1–4. 49) Markov MS. 2007 Pulsed electromagnetic field therapy: History, state of the art and future. The Environmentalist 27:465-475. 50) Nittby H, Grafstrom G, Eberhardt JL, Malmgren L, Brun A, Persson BR, Salford, LG. 2008 Radiofrequency and extremely low frequency electromagnetic field effects on the bloodbrain barrier. Electromag Biol Med 2008; 27:103-126. 51) Hazout A, Menezo Y, Madelenat P, Yazbeck C, Selva J, Cohen-Bacrie P. 2008 [Causes and clinical implications of sperm DNA damages]. [Article in French] Gynecol Obstet Fertil 36:1109-1117. 52) Hardell, L., Sage, C. 2008. Biological effects from electromagnetic field exposure and public exposure standards. Biomed. Pharmacother. 62, 104-109. 53) Genuis SJ. 2008 Fielding a current idea: exploring the public health impact of electromagnetic radiation. Public Health 122:113-124. 54) Johansson O. 2009 Disturbance of the immune system by electromagnetic fields-A potentially underlying cause for cellular damage and tissue repair reduction which could lead to disease and impairment. Pathophysiology 16:157-177. 55) Blackman C. 2009 Cell phone radiation: Evidence from ELF and RF studies supporting more inclusive risk identification and assessment. Pathophysiology. 2009 Aug;16(2-3):205-216 56) Balmori A. 2009 Electromagnetic pollution from phone masts. Effects on wildlife. Pathophysiology 16:191-199. 57) Davanipour Z, Sobel E. 2009 Long-term exposure to magnetic fields and the risks of Alzheimer's disease and breast cancer: Further biological research. Pathophysiology 16:149-156. 58) Desai NR, Kesari KK, Agarwal A. 2009 Pathophysiology of cell phone radiation: oxidative stress and carcinogenesis with focus on the male reproductive system. Reproduct Biol Endocrinol 7:114. 59) Khurana VG, Teo C, Kundi M, Hardell L, Carlberg M. 2009 Cell phones and brain tumors: a review including the long-term epidemiologic data. Surg Neurol 72:205-214. 60) Martin Blank, Reba Goodman. 2009 Electromagnetic fields stress living cells. Pathophysiology 16:71-78. 61) Phillips JL, Singh NP, Lai H. 2009 Electromagnetic fields and DNA damage. Pathophysiology 16:79-88. 62) Makker K, Varghese A, Desai NR, Mouradi R, Agarwal A. 2009 Cell phones: modern man's nemesis? Reprod Biomed Online 18:148-157. 63) Ruediger HW. 2009 Genotoxic effects of radiofrequency electromagnetic fields. Pathophysiology. 16:89-102. 64) Yakymenko I, Sidorik E. 2010 Risks of carcinogenesis from electromagnetic radiation and mobile telephony devices. Exp Oncol 32:729-736. 65) Carpenter DO. 2010 Electromagnetic fields and cancer: the cost of doing nothing. Rev Environ Health 25:75-80. 66) Khurana, V. G., Hardell, L., Everaert, J., Bortkiewicz, A., Carlberg, M., Ahonen, M. 2010 Epidemiological evidence for a health risk from mobile phone base stations. Int. J. Occup. Environ. Health 16, 263-267. 67) Giuliani L, Soffriti M (Eds). 2010 NON-THERMAL EFFECTS AND MECHANISMS OF INTERACTION BETWEEN ELECTROMAGNETIC FIELDS AND LIVING MATTER, RAMAZZINI INSTITUTE EUR. J. ONCOL. LIBRARY Volume 5, National Institute for the Study and Control of Cancer and Environmental Diseases “Bernardino Ramazzini” Bologna, Italy 2010, 400 page monograph. 68) Fragopoulou A, Grigoriev Y, Johansson O, Margaritis LH, Morgan L, Richter E, Sage C. Scientific panel on electromagnetic field health risks: consensus points, recommendations, and rationales. Rev. Environ. Health 25, 307-317. 69) Batista Napotnik T, Reberšek M, Vernier PT, Mali B, Miklavčič D. 2010 Effects of high voltage nanosecond electric pulses on eukaryotic cells (in vitro): A systematic review. Bioelectrochemistry 110:1-12. 70) Levitt, B. B., Lai, H. 2010. Biological effects from exposure to electromagnetic radiation emitted by cell tower base stations and other antenna arrays. Environ. Rev. 18, 369-395. 71) Yu Y, Yao K. 2010 Non-thermal cellular effects of low power microwave radiation on the lens and lens epithelial cells. J Int Med Res 38:729-736. 72) Yakymenko, I., Sidorik, E., Kyrylenko, S., Chekhun, V. 2011. Long-term exposure to microwave radiation provokes cancer growth: evidences from radars and mobile communication systems. Exp. Oncol. 33(2), 62-70. 73) Kesari KK, Kuman S, Behari J. 2011 Effects of radiofrequency electromagnetic wave exposure from cellular phones on reproductive pattern in male Wistar rats. Appl Biochem Biotechnol 164:546-549. 74) Panagopoulos DJ. 2011 Analyzing the health impacts of modern telecommunication microwaves. Chapter 1 in Advances in Biology and Medicine, Vol. 17, Leon V. Berhardt, Ed., Nova Science Publishers. 75) Schidt-Rohlfing B, Silny J, Gavenis K, et al. 2011 Electromagnetic fields, electric current and bone healing – what is the evidence? Z Orthop Unfall. 149: 265–270. 76) Chalidis B, Sachinis N, Assiotis A, et al. 2011 Stimulation of bone formation and fracture healing with pulsed electromagnetic fields: biologic responses and clinical implica- tions. Int J Immunopathol Pharmacol. 2011; 24(1 Suppl. 2): 17020. 77) Pilla A, Fitzsimmons R, Muehsam D, et al. 2011 Electromagnetic fields as first messenger in biological signaling: application to calmodulin-dependent signaling in tissue repair. Biochim Biophys Acta 1810: 1236–1245. 78) Yakimenko IL, Sidorik EP, Tsybulin AS. 2011 [Metabolic changes in cells under electromagnetic radiation of mobile communication systems]. [Article in Russian] Ukr Biokhim Zh 83:20-28. 79) La Vignera, Condorelli RA, Vicari E, D’Agata R, Calogero AE. 2012 Effects of the exposure to mobile phones on male reproduction: a review of the literature. J Androl 33:350-356. 80) Zhong C, Zhao TF, Xu ZJ, et al. 2012 Effects of electromagnetic fields on bone regeneration in experimental and clinical studies: a review of the literature. Chin Med J 125: 367–372. 81) Biointiative Working Group, David Carpenter and Cindy Sage (eds). 2012 Bioinitiative 2012: A rationale for biologically-based exposure standards for electromagnetic radiation. http://www.bioinitiative.org/participants/why-we-care/ 82) Gye MC, Park CJ. 2012 Effect of electromagnetic field exposure on the reproductive system. Clin Exp Reprod Med 39:1-9. 83) Trošić I, Pavičić I, Marjanović AM, Bušljeta I. 2012 Non-thermal biomarkers of exposure to radiofrequency/microwave radiation. Arh Hig Rada Toksikol 63 Suppl 1:67-73. 84) Consales, C., Merla, C., Marino, C., et al. 2012. Electromagnetic fields, oxidative stress, and neurodegeneration. Int. J. Cell Biol. 2012: 683897. 85) Havas, M. 2013. Radiation from wireless technology affects the blood, the heart, and the autonomic nervous system. Rev. Environ. Health. 28(Nov 2013), 75-84. 86) Herbert, M. R., Sage, C. 2013 Autism and EMF? Plausibility of a pathophysiological link – Part I. Pathophysiology 20, 191-209. 87) Herbert, M. R., Sage, C. 2013. Autism and EMF? Plausibility of a pathophysiological link part II. Pathophysiology 20, 211-234. 88) Jayasanka SMDH, Asaeda T. 2013 The significance of microwaves in the environment and its effects on plants. Envron Rev 22:220-228. 89) Kesari KK, Siddiqui MH, Meena R, Verma HN, Kumar S. 2013 Cell phone radiation exposure on brain and associated biological systems. Indian J Exp Biol 51:187-200. 90) Warnke U, Hensinger P. 2013 Increasing incidence of burnout due to magnetic fields of cell phone networks and other wireless communication technologies. Umwelt Medizin Gesellshaft 26: 31-38. 91) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2013. Evaluation of specific absorption rate as a dosimetric quantity for electromagnetic fields bioeffects. PloS ONE 8(6): e62663. doi:10:1371 92) Carpenter DO. 2013. Human disease resulting from exposure to electromagnetic fields. Rev Environ Health. 2013;28(4):159-72. 93) Ledoigt G, Belpomme D. 2013 Cancer induction molecular pathways and HF-EMF irradiation. Adv Biol Chem 3:177-186. 94) Pall, ML. 2013. Electromagnetic fields act via activation of voltage-gated calcium channels to produce beneficial or adverse effects. J. Cell. Mol. Med. 17:958-965. 95) Pilla, AA. 2013 Nonthermal electromagnetic fields: from first messenger to therapeutic applications. Electromagn. Biol. Med. 32, 123-136. 96) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2013. Evaluation of specific absorption rate as a dosimetric quantity for electromagnetic fields bioeffects. PloS ONE 8(6): e62663. doi:10:1371 97) Halgamuge MN. 2013 Pineal melatonin level disruption in humans due to electromagnetic fields and ICNIRP limits. Radiat Prot Dosimetr 154: 405-416 98) Szmigielski S. 2013 Reaction of the immune system to low-level RF/MW exposures. Sci Total Environ 2013 Jun 1;454-455:393-400. 99) Hardell L, Carlberg M, Hansson Mild K. 2013 Use of mobile phones and cordless phones is associated with increased risk for glioma and acoustic neuroma. Pathophysiology 2013;20(2):85-110. 100) Davis DL, Kesari S, Soskolne CL, Miller AB, Stein Y. 2013 Swedish review strengthens grounds for concluding that radiation from cellular and cordless phones is a probable human carcinogen. Pathophysiology 20:123-129. 101) Naziroglu M, Yuksel M, Kose SA, Ozkaya MO. 2013 Recent reports of Wi-Fi and mobile phone-induced radiation on oxidative stress and reproductive signaling pathways in females and males. [review] J Membr Biol 246 (12): 869-875. 102) Adams, J. A., Galloway, T. S., Mondal, D., Esteves, S. C. 2014 Effect of mobile telephones on sperm quality: A systematic review and meta-analysis. Environment. Int. 70, 106-112. 103) Murbach, M., Neufeld, E., Christopoulou, M., Achermann, P., Kuster, N. 2014. Modeling of EEG electrode artifacts and thermal ripples in human radiofrequency exposure studies. Bioelectromagnetics 35, 273-283. 104) Lewczuk B, Redlarski G, Zak A, Ziółkowska N, Przybylska-Gornowicz B, Krawczuk M. 2014 Influence of electric, magnetic, and electromagnetic fields on the circadian system: current stage of knowledge. Biomed Res Int. 2014;2014:169459. doi: 10.1155/2014/169459. Epub 2014 Jul 22. 105) Van Boxem K, Huntoon M, Van Zundert J, Patijn J, van Kleef M, Joosten EA. 2014 Pulsed radiofrequency: a review of the basic science as applied to the pathophysiology of radicular pain: a call for clinical translation. Reg Anesth Pain Med. 2014 Mar-Apr;39(2):14959. 106) Liu K, Li Y, Zhang G, Liu J, Cao J, Ao L, Zhang S. 2014 Association between mobile phone use and semen quality: a systematic review and meta-analysis. Andrology 2:491-501. 107) Pilla, AA 2015 Pulsed electromagnetic fields: from signaling to healing. In: Markov, M. S., Ed. 2015. Electromagnetic Fields in Biology and Medicine. CRC Press, Taylor and Francis Group, Boca Raton, FL. , pp. 29-40.108) Belyaev, I. 2015. Biophysical mechanisms for nonthermal microwave effects. In: Electromagnetic Fields in Biology and Medicine, Marko S. Markov, ed, CRC Press, New York, pp 49-67. (Please note: There are probably a dozen other reviews that from this volume that might be included here on non-thermal effects) 109) Sangün Ö, Dündar B, Çömlekçi S, Büyükgebiz A. 2015 The Effects of Electromagnetic Field on the Endocrine System in Children and Adolescents. Pediatr Endocrinol Rev 13:531-545. 110) Pall, M. L. 2015. Scientific evidence contradicts findings and assumptions of Canadian Safety Panel 6: microwaves act through voltage-gated calcium channel activation to induce biological impacts at non-thermal levels, supporting a paradigm shift for microwave/lower frequency electromagnetic field action. Rev. Environ. Health 3, 99-116. 111) Panagopoulos, D. J., Johansson, O., Carlo, G. L. 2015. Real versus simulated mobile phone exposures in experimental studies. BioMed. Res. Int. 2015, article ID 607053, 8 pages. 112) Mahdavi M, Yekta R, Tackallou SH. 2015 Positive correlation between ELF and RF electromagnetic fields on cancer risk. J Paramed Sci 6(3), ISSN 2008-4978. 113) Morgan LL, Miller AB, Sasco A, Davis DL. 2015 Mobile phone radiation causes brain tumors and should be classified as a probable human carcinogen (2A). Int J Oncol 46(5): 1865-71. 114) Vadalà M, Vallelunga A, Palmieri L, Palmieri B, Morales-Medina JC, Iannitti T. 2015 Mechanisms and therapeutic applications of electromagnetic therapy in Parkinson's disease. Behav Brain Funct. 2015 Sep 7;11:26. doi: 10.1186/s12993-015-0070-z. 115) Lim R, Lee SW, Tan PY, Liong ML, Yuen KH. 2015 Efficacy of electromagnetic therapy for urinary incontinence: A systematic review. Neurourol Urodyn 34(8):713-722. 116) Hedendahl L, Carlberg M, Hardell L. 2015 Electromagnetic hypersensitivity – an increasing challenge to the medical profession. Rev Environ Health 30:209-215. 117) Carpenter DO. 2015 The microwave syndrome or electro-hypersensitivity: historical background. Rev Environ Health. 30:217-222. 118) Yakymenko I, Tsybulin O, Sidorik E, Henshel D, Kyrylenko O, Kysylenko S. 2015 Oxidative mechanisms of biological activity of low-intensity radiofrequency radiation. Electromagnetic Biol Med: Early Online 1-16. ISSN: 1536-8378. 119) Panagopoulos DJ, Johansson O, Carlo GL. 2015 Polarization: A Key Difference between Man-made and Natural Electromagnetic Fields, in regard to Biological Activity. Sci Rep. 2015 Oct 12;5:14914. doi: 10.1038/srep14914. 120) Sage C. 2015 The implications of non-linear biological oscillations on human electrophysiology for electrohypersensitivity (EHS) and multiple chemical sensitivity (MCS). Rev Environ Health. 2015;30(4):293-303. 121) Eghlidospour M, Mortazavi SM, Yousefi F, Mortazavi SA. 2015 New Horizons in Enhancing the Proliferation and Differentiation of Neural Stem Cells Using Stimulatory Effects of the Short Time Exposure to Radiofrequency Radiation. J Biomed Phys Eng. 2015 Sep 1;5(3):95-104. eCollection 2015 Sep. 122) Kaszuba-Zwoińska J, Gremba J, Gałdzińska-Calik B, Wójcik-Piotrowicz K, Thor PJ. 2015 Electromagnetic field induced biological effects in humans. Przegl Lek. 2015;72(11):636-41. 123) K Sri N. 2015 Mobile Phone Radiation: Physiological & Pathophysiologcal Considerations. Indian J Physiol Pharmacol. 2015 Apr-Jun;59(2):125-35. 124) Redmayne M, Johansson O. 2015 Radiofrequency exposure in young and old: different sensitivities in light of age-relevant natural differences. Rev Environ Health 30: 323-335. 125) Pall, ML. 2016. Microwave frequency electromagnetic fields (EMFs) produce widespread neuropsychiatric effects including depression. J. Chem. Neuroanat. 75(Pt B):4351. 126) Warille AA, Onger ME, Turkmen AP, Deniz ÖG, Altun G, Yurt KK, Altunkaynak BZ, Kaplan S. 2016 Controversies on electromagnetic field exposure and the nervous systems of children. Histol Histopathol 31(5):461-468.27) Vian A, Davies E, Gendraud M, Bonnet P. 2016 Plant Responses to High Frequency Electromagnetic Fields. Biomed Res Int. 2016;2016:1830262. doi: 10.1155/2016/1830262. Epub 2016 Feb 14. 128) Kaplan S, Deniz OG, Önger ME, Türkmen AP, Yurt KK, Aydın I, Altunkaynak BZ, Davis D. 2016 Electromagnetic field and brain development. J Chem Neuroanat 75(Pt B):52-61. 129) Altunkaynak BZ, Altun G, Yahyazadeh A, Kaplan AA, Deniz OG, Türkmen AP, Önger ME, Kaplan S. 2016 Different methods for evaluating the effects of microwave radiation exposure on the nervous system. J Chem Neuroanat. 2016 Sep;75(Pt B):62-9. 130) Dasdag S, Akdag MZ. 2016 The link between radiofrequencies emitted from wireless technologies and oxidative stress. J Chem Neuroanat. 2016 Sep;75(Pt B):85-93. 131) Terzi M, Osberk B, Deniz OG, Kaplan S. 2016 The role of electromagnetic fields in neurological disorders. . J Chem Neuroanat. 2016 Sep;75(Pt B):77-84. 132) Maziarz A, Kocan B, Bester M, Budzik S, Cholewa M, Ochiya T, Banas A. 2016 How electromagnetic fields can influence adult stem cells: positive and negative impacts. Stem Cell Res Ther 2016 Apr 18;7(1):54. doi: 10.1186/s13287-016-0312-5. 133) Soghomonyan D, Trchounian K, Trchounian A. 2016 Millimeter waves or extremely high frequency electromagnetic fields in the environment: what are their effects on bacteria? Appl Microbiol Biotechnol. 100:4761-4771. 134) Maes A, Verschaeve L. 2016 Genetic damage in humans exposed to extremely lowfrequency electromagnetic fields. Arch Toxicol. 2016 Jun 23. [Epub ahead of print] 135) Belyaev I, Dean A, Eger H, Hubmann G, Jandrisovits R, Johansson O, Kern M, Kundi M, Lercher P, Mosgöller W, Moshammer H, Müller K, Oberfeld G, Ohnsorge P, Pelzmann P, Scheingraber C, Thill R. 2016 EUROPAEM EMF Guideline 2016 for the prevention, diagnosis and treatment of EMF-related health problems and illnesses. Rev. Environ. Health DOI 10.1515/reveh-2016-0011. 136) Pall ML. 2016 Electromagnetic fields act similarly in plants as in animals: Probable activation of calcium channels via their voltage sensor. Curr Chem Biol 10:74-82. 137) Medeiros LN, Sanchez TG. 2016 Tinnitus and cell phones: the role of electromagnetic radiofrequency radiation. Braz J Otorhinolaryngol. 2016 Jan-Feb;82(1):97104. 138) Starkey SJ. 2016 Inaccurate official assessment of radiofrequency safety by the Advisory Group on Non-ionising Radiation. Rev Environ Health 31:493-503. 139) Hecht K. 2016 Health Implications of Long-term Exposure to Electrosmog: Effects of Wireless Communication Technologies, pp 1-64. Brochure 6 of A Brochure Series of the Competence Initiative for the Protection of Humanity, the Environment and Democracy E.V. URL: http://kompetenzinitiative.net/KIT/wp-content/uploads/2016/07/KI_Brochure6_K_Hecht_web.pdf 140) Asghari A, Khaki AA, Rajabzadeh A, Khaki A. 2016 A review on electromagnetic fields (EMFs) and the reproductive system. Electron Physician. 2016 Jul 25;8(7):2655-62. 141) Houston BJ, Nixon B, King BV, De Iuliis GN, Aitken RJ. 2016 The effects of radiofrequency electromagnetic radiation on sperm function. Reproduction. 2016 Dec;152(6):R263-R276. 142) Halgamuge MN. 2017 Review: Weak radiofrequency radiation exposure from mobile phone radiation on plants. Electromagn Biol Med. 2017;36(2):213-235. 143) Bortkiewicz A, Gadzicka E, Szymczak W. 2017 Mobile phone use and risk for intracranial tumors and salivary gland tumors - A meta-analysis. Int J Occup Med Environ Health. 2017 Feb 21;30(1):27-43. 144) Carlberg M, Hardell L. 2017 Evaluation of Mobile Phone and Cordless Phone Use and Glioma Risk Using the Bradford Hill Viewpoints from 1965 on Association or Causation. BioMed Res Int 2017, Article ID 9218486, https://doi.org/10.1155/2017/9218486 145) Bielsa-Fernández P, Rodríguez-Martín B. 2017 [Association between radiation from mobile phones and tumour risk in adults]. Gac Sanit. 2017 Apr 12. pii: S02139111(17)30083-3. doi: 10.1016/j.gaceta.2016.10.014. [Epub ahead of print] 146) Alegría-Loyola MA, Galnares-Olalde JA, Mercado M. 2017 [Tumors of the central nervous system]. Rev Med Inst Mex Seguro Soc. 2017 May-Jun;55(3):330-340. 47) Miah T, Kamat D. 2017 Current Understanding of the Health Effects of Electromagnetic Fields. Pediatr Ann. 2017 Apr 1;46(4):e172-e174. doi: 10.3928/1938235920170316-01. 148) Facchini G, Spinnato P, Guglielmi G, Albisinni U, Bazzocchi A. 2017 A comprehensive review of pulsed radiofrequency in the treatment of pain associated with different spinal conditions. Br J Radiol. 2017 May;90(1073):20150406. doi: 10.1259/bjr.20150406. Epub 2017 Feb 10. 149) Kim K, Jo D, Kim E. 2017 Pulsed Radiofrequency to the Dorsal Root Ganglion in Acute Herpes Zoster and Postherpetic Neuralgia. Pain Physician. 2017 Mar;20(3):E411E418. 150) Prasad M, Kathuria P, Nair P, Kumar A, Prasad K. 2017 Mobile phone use and risk of brain tumours: a systematic review of association between study quality, source of funding, and research outcomes. Neurol Sci. 2017 Feb 17. doi: 10.1007/s10072-017-2850-8. [Epub ahead of print]. 151) Bandara P, Weller S. 2017 Cardiovascular disease: Time to identify emerging environmental factors. Eur J Prevent Cardiol 24(17):1819-1823. 152) Wang J, Su H, Xie W, Yu S. Mobile Phone Use and The Risk of Headache: A Systematic Review and Meta-analysis of Cross-sectional Studies. Sci Rep. 2017 Oct 3;7(1):12595. doi: 10.1038/s41598-017-12802-9. 153) .Mishra SK, Chowdhary R, Kumari S, Rao SB. 2017 Effect of Cell Phone Radiations on Orofacial Structures: A Systematic Review. J Clin Diagn Res. 2017 May;11(5):ZE01-ZE05. doi: 10.7860/JCDR/2017/26547.9883. Epub 2017 May 1 154) Hardell L. 2017 World Health Organization, radiofrequency radiation and health – a hard nut to crack (Review). Int J Oncol 51:405-413. 155) Wang H, Zhang X. 2017 Magnetic Fields and Reactive Oxygen Species. Int J Mol Sci. 2017 Oct 18;18(10). pii: E2175. doi: 10.3390/ijms18102175.
Functional Brain MRI in Patients Complaining of Electrohypersensitivity After Long Term Exposure to Electromagnetic Fields
Gunnar Heuser* and Sylvia A. Heuser
DOI 10.1515/reveh-2017-0014
Received April 3, 2017; accepted May 25, 2017; previously published online July 5, 2017
https://www.degruyter.com/downloadpdf/j/reveh.2017.32.issue-3/reveh-2017-0014/reveh-2017-0014.pdf
Abstract
Introduction: Ten adult patients with electromagnetic hypersensitivity underwent functional magnetic resonance imaging (fMRI) brain scans. All scans were abnormal with abnormalities which were consistent and similar. It is proposed that fMRI brain scans be used as a diagnostic aid for determining whether or not a patient has electromagnetic hypersensitivity. Over the years we have seen an increasing number of patients who had developed multi system complaints after long term repeated exposure to electromagnetic fields (EMFs). These complaints included headaches, intermittent cognitive and memory problems, intermittent disorientation, and also sensitivity to EMF exposure. Regular laboratory tests were within normal limits in these patients. The patients refused to be exposed to radioactivity. This of course ruled out positron emission tomography (PET) and single-photon emission computed tomography (SPECT) brain scanning. This is why we ordered fMRI brain scans on these patients. We hoped that we could document objective abnormalities in these patients who had often been labeled as psychiatric cases.
Materials and methods: Ten patients first underwent a regular magnetic resonance imaging (MRI) brain scan, using a 3 Tesla Siemens Verio MRI open system. A functional MRI study was then performed in the resting state using the following sequences:
1. A three-dimensional, T1-weighted, gradient-echo (MPRAGE)
2. Resting state network. The echo-planar imaging (EPI) sequences for this resting state blood oxygenation level
dependent (BOLD) scan were then post processed on a 3D workstation and the independent component analysis was performed separating out the various networks.
3. Arterial spin labeling.
4. Tractography and fractional anisotropy.
Results: All ten patients had abnormal functional MRI brain scans. The abnormality was often described as hyper connectivity of the anterior component of the default mode in the medial orbitofrontal area. Other abnormalities were usually found. Regular MRI studies of the brain were mostly unremarkable in these patients.
Conclusion: We propose that functional MRI studies should become a diagnostic aid when evaluating a patient who claims electrohypersensitivity (EHS) and has otherwise normal studies. Interestingly, the differential diagnosis for the abnormalities seen on the fMRI includes head injury. It turns out that many of our patients indeed had a history of head injury which was then followed sometime later by the development of EHS. Many of our patients also had a history of exposure to potentially neurotoxic chemicals, especially mold. Head injury and neurotoxic chemical exposure may make a patient more vulnerable to develop EHS.
Keywords: electrohypersensitivity (EHS); electromagnetic field (EMF); fMRI; multiple chemical sensitivity (MCS).
Introduction
In the past the senior author (G.H.) practiced clinical toxicology and in that capacity saw more than 1000 patients who had suffered exposure to toxic chemicals. Their impairment was often neurologic with loss of memory function, headaches, intermittent confusion, problems with balance, and other symptoms. This impairment had persisted, at times for years after exposure to these toxic chemicals had ceased. Some of these patients had developed sensitivity to even small amounts of chemicals resulting in multiple chemical sensitivity (MCS). More than 60 patients were eventually studied and the results were published in a peer reviewed journal [1]. All of these patients had single-photon emission computed tomography (SPECT) brain scans all of which were abnormal. Additional studies were then performed and published [2, 3].
More recently we began to see patients who reported significant reactions to even small amounts of electromagnetic fields (EMFs). Some of these patients had in the past been seen for problems with chemical exposure and had now developed electrohypersensitivity (EHS). Some of these patients also gave a history of head injury.
Electrohypersensitivity has since been acknowledged by the medical profession since it demands more and more attention and evaluation [4–7]. The syndrome has now been called EHS.
Patients with EHS develop multi-system complaints on exposure to currents emitted by cell phones, cell phone towers, smart meters, power-lines and other sources of EMFs.
In this paper we present patients with EHS who had undergone functional brain MRI studies because of their complaints which were mostly neurological after expo- sure: memory and cognitive impairment, attention deficit disorder, changes in behavior, and other symptoms. They presented with a history of long term exposure to EMFs followed by development of EHS.
Every patient included in this paper reported significant symptomatology which served to arrive at a diagnosis of EHS. Symptoms developed upon exposure and usually diminished or disappeared when removed from EMF source. Multi-symptoms included headaches, impairment of cognitive function, tremors, weakness, and others. Multi-system complaints were triggered by exposure to cell phones, cell phone towers, smart meters, wi-fi, and other sources (see description of individual cases).
A careful and thorough lab evaluation ruled out dis- eases which often cause multi system complaints e.g. thyroid problems, diabetes, autoimmune disease, chronic infections and other conditions. Patients often provided pictures of nearby cell phone towers, smart meters and other sources of EMFs to document their claim.
Methodology
Table 1: Patient population.
DOI 10.1515/reveh-2017-0014
Received April 3, 2017; accepted May 25, 2017; previously published online July 5, 2017
https://www.degruyter.com/downloadpdf/j/reveh.2017.32.issue-3/reveh-2017-0014/reveh-2017-0014.pdf
Abstract
Introduction: Ten adult patients with electromagnetic hypersensitivity underwent functional magnetic resonance imaging (fMRI) brain scans. All scans were abnormal with abnormalities which were consistent and similar. It is proposed that fMRI brain scans be used as a diagnostic aid for determining whether or not a patient has electromagnetic hypersensitivity. Over the years we have seen an increasing number of patients who had developed multi system complaints after long term repeated exposure to electromagnetic fields (EMFs). These complaints included headaches, intermittent cognitive and memory problems, intermittent disorientation, and also sensitivity to EMF exposure. Regular laboratory tests were within normal limits in these patients. The patients refused to be exposed to radioactivity. This of course ruled out positron emission tomography (PET) and single-photon emission computed tomography (SPECT) brain scanning. This is why we ordered fMRI brain scans on these patients. We hoped that we could document objective abnormalities in these patients who had often been labeled as psychiatric cases.
Materials and methods: Ten patients first underwent a regular magnetic resonance imaging (MRI) brain scan, using a 3 Tesla Siemens Verio MRI open system. A functional MRI study was then performed in the resting state using the following sequences:
1. A three-dimensional, T1-weighted, gradient-echo (MPRAGE)
2. Resting state network. The echo-planar imaging (EPI) sequences for this resting state blood oxygenation level
dependent (BOLD) scan were then post processed on a 3D workstation and the independent component analysis was performed separating out the various networks.
3. Arterial spin labeling.
4. Tractography and fractional anisotropy.
Results: All ten patients had abnormal functional MRI brain scans. The abnormality was often described as hyper connectivity of the anterior component of the default mode in the medial orbitofrontal area. Other abnormalities were usually found. Regular MRI studies of the brain were mostly unremarkable in these patients.
Conclusion: We propose that functional MRI studies should become a diagnostic aid when evaluating a patient who claims electrohypersensitivity (EHS) and has otherwise normal studies. Interestingly, the differential diagnosis for the abnormalities seen on the fMRI includes head injury. It turns out that many of our patients indeed had a history of head injury which was then followed sometime later by the development of EHS. Many of our patients also had a history of exposure to potentially neurotoxic chemicals, especially mold. Head injury and neurotoxic chemical exposure may make a patient more vulnerable to develop EHS.
Keywords: electrohypersensitivity (EHS); electromagnetic field (EMF); fMRI; multiple chemical sensitivity (MCS).
Introduction
In the past the senior author (G.H.) practiced clinical toxicology and in that capacity saw more than 1000 patients who had suffered exposure to toxic chemicals. Their impairment was often neurologic with loss of memory function, headaches, intermittent confusion, problems with balance, and other symptoms. This impairment had persisted, at times for years after exposure to these toxic chemicals had ceased. Some of these patients had developed sensitivity to even small amounts of chemicals resulting in multiple chemical sensitivity (MCS). More than 60 patients were eventually studied and the results were published in a peer reviewed journal [1]. All of these patients had single-photon emission computed tomography (SPECT) brain scans all of which were abnormal. Additional studies were then performed and published [2, 3].
More recently we began to see patients who reported significant reactions to even small amounts of electromagnetic fields (EMFs). Some of these patients had in the past been seen for problems with chemical exposure and had now developed electrohypersensitivity (EHS). Some of these patients also gave a history of head injury.
Electrohypersensitivity has since been acknowledged by the medical profession since it demands more and more attention and evaluation [4–7]. The syndrome has now been called EHS.
Patients with EHS develop multi-system complaints on exposure to currents emitted by cell phones, cell phone towers, smart meters, power-lines and other sources of EMFs.
In this paper we present patients with EHS who had undergone functional brain MRI studies because of their complaints which were mostly neurological after expo- sure: memory and cognitive impairment, attention deficit disorder, changes in behavior, and other symptoms. They presented with a history of long term exposure to EMFs followed by development of EHS.
Every patient included in this paper reported significant symptomatology which served to arrive at a diagnosis of EHS. Symptoms developed upon exposure and usually diminished or disappeared when removed from EMF source. Multi-symptoms included headaches, impairment of cognitive function, tremors, weakness, and others. Multi-system complaints were triggered by exposure to cell phones, cell phone towers, smart meters, wi-fi, and other sources (see description of individual cases).
A careful and thorough lab evaluation ruled out dis- eases which often cause multi system complaints e.g. thyroid problems, diabetes, autoimmune disease, chronic infections and other conditions. Patients often provided pictures of nearby cell phone towers, smart meters and other sources of EMFs to document their claim.
Methodology
Table 1: Patient population.
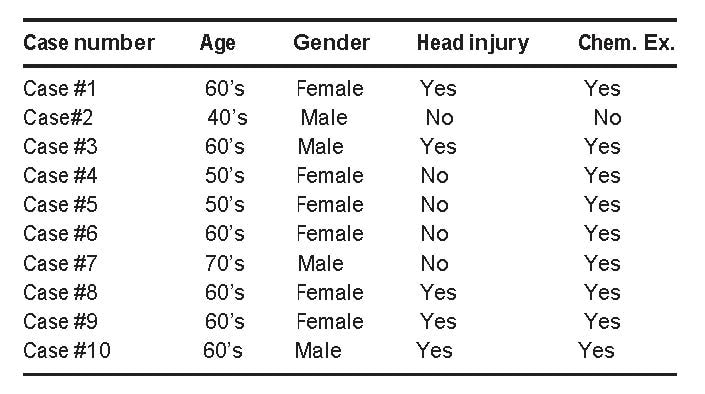
scans were then post processed on a 3D workstation and the independent component analysis was performed separating out the various networks.
3. Arterial spin labeling.
4. Tractography and fractional anisotropy (Table 1).
Results
3. Arterial spin labeling.
4. Tractography and fractional anisotropy (Table 1).
Results
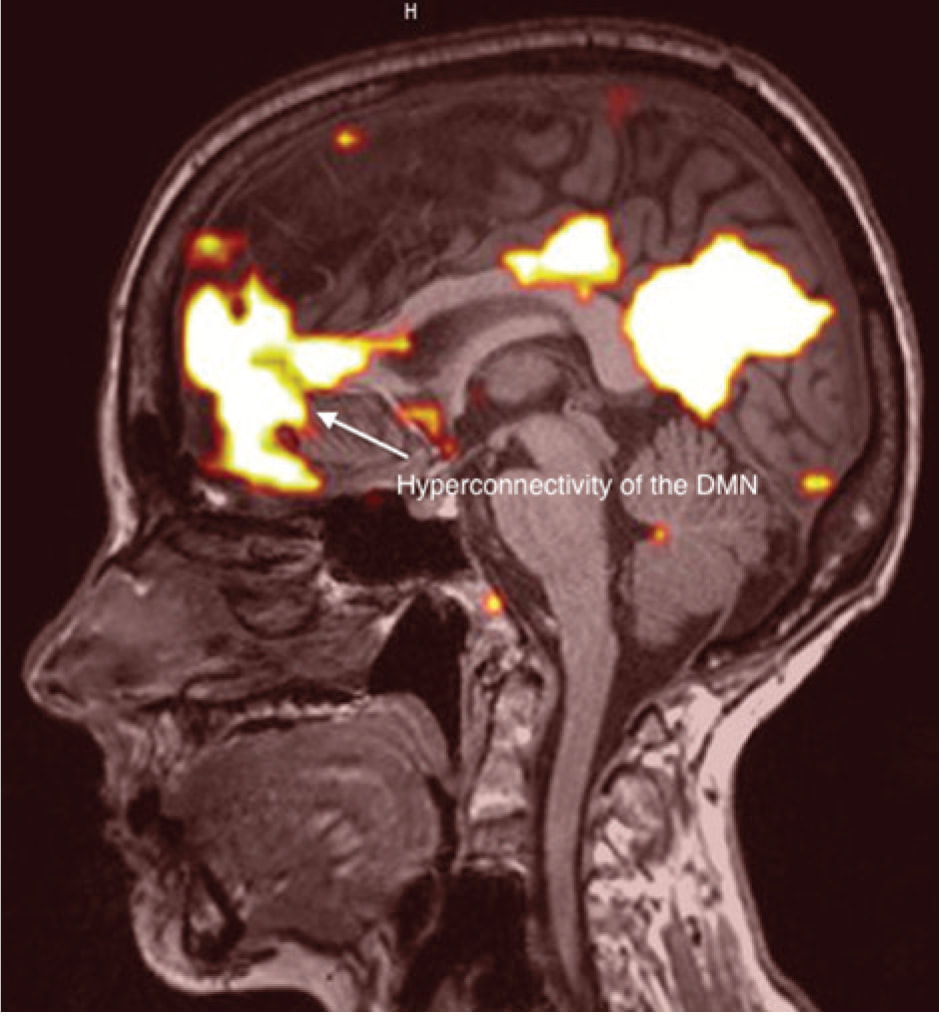
Figure 1: Lateral view of case no. 1.
Case 1. This right handed patient was in her early sixties when she was evaluated. Whenever exposed to EMFs she developed cognitive and memory problems as well as a sense of malaise to the point of inability to function. Her EHS developed over the years. Her history includes multiple head injuries and also exposure to toxic chemicals, including mold, eventually resulting in multiple chemical sensitivity (MCS)
The fMRI showed severely abnormal default mode network (DMN) with hyper connectivity of the anterior component in the medial orbitofrontal area, also decrease of white matter tracts within the right frontal lobe, and finally decreased flow and/or metabolism within bifrontal lobes (Figure 1).
Case 1. This right handed patient was in her early sixties when she was evaluated. Whenever exposed to EMFs she developed cognitive and memory problems as well as a sense of malaise to the point of inability to function. Her EHS developed over the years. Her history includes multiple head injuries and also exposure to toxic chemicals, including mold, eventually resulting in multiple chemical sensitivity (MCS)
The fMRI showed severely abnormal default mode network (DMN) with hyper connectivity of the anterior component in the medial orbitofrontal area, also decrease of white matter tracts within the right frontal lobe, and finally decreased flow and/or metabolism within bifrontal lobes (Figure 1).
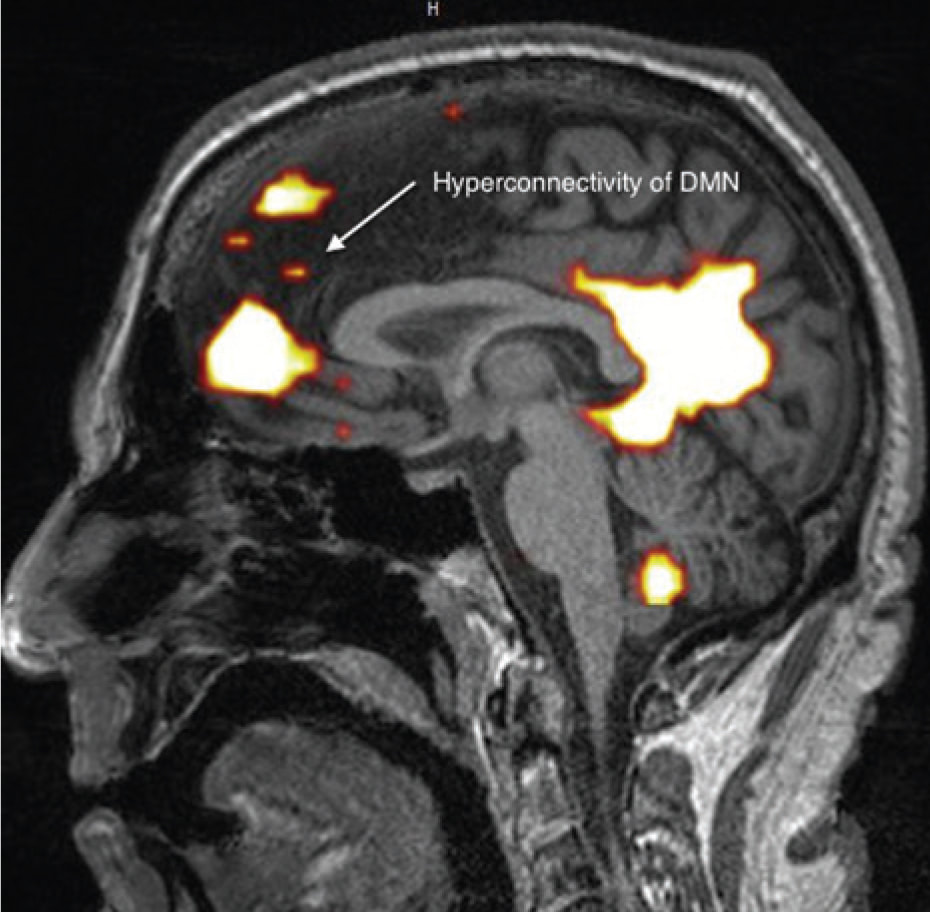
Figure 2: Lateral view of case no. 2. Case 2. This right handed patient was in his forties when evaluated. Several years before he had an abnormal SPECT brain scan and an abnormal neuropsychological test result suggesting attention deficit disorder (ADD). For approximately 11 years he had worked as an air conditioning expert, working on the roofs of many commercial buildings, thus being exposed to EMFs. He developed cognitive and memory problems, impaired coordination and balance, insomnia, chronic fatigue, and finally EHS. In addition he was diagnosed to have bi-lateral cataracts impairing his vision. His history is negative for head injury and toxic chemical exposure.
The fMRI showed abnormality of the DMN with increased hyperconnectivity of the anterior component.
Fractional anisotropy was found to be decreased in the corpus callosum (Figure 2).
The fMRI showed abnormality of the DMN with increased hyperconnectivity of the anterior component.
Fractional anisotropy was found to be decreased in the corpus callosum (Figure 2).

Figure 3: Lateral view of case no. 3.
Case 3. This right handed patient was in his sixties when being evaluated. He had worked in a high voltage environment as a journeyman lineman for more than 30 years, evaluating and treating problems in that environment.
Eventually, he developed a seizure disorder with loss of consciousness. His seizures subsided when he was off work and returned when he returned to work.
He had a concussion in his teenage years. He had not been exposed to mold.
The fMRI showed fragmentation of the anterior component of the DMN, also decreased fractional anisotropy, predominantly in the corpus callosum (Figure 3).
Case 3. This right handed patient was in his sixties when being evaluated. He had worked in a high voltage environment as a journeyman lineman for more than 30 years, evaluating and treating problems in that environment.
Eventually, he developed a seizure disorder with loss of consciousness. His seizures subsided when he was off work and returned when he returned to work.
He had a concussion in his teenage years. He had not been exposed to mold.
The fMRI showed fragmentation of the anterior component of the DMN, also decreased fractional anisotropy, predominantly in the corpus callosum (Figure 3).
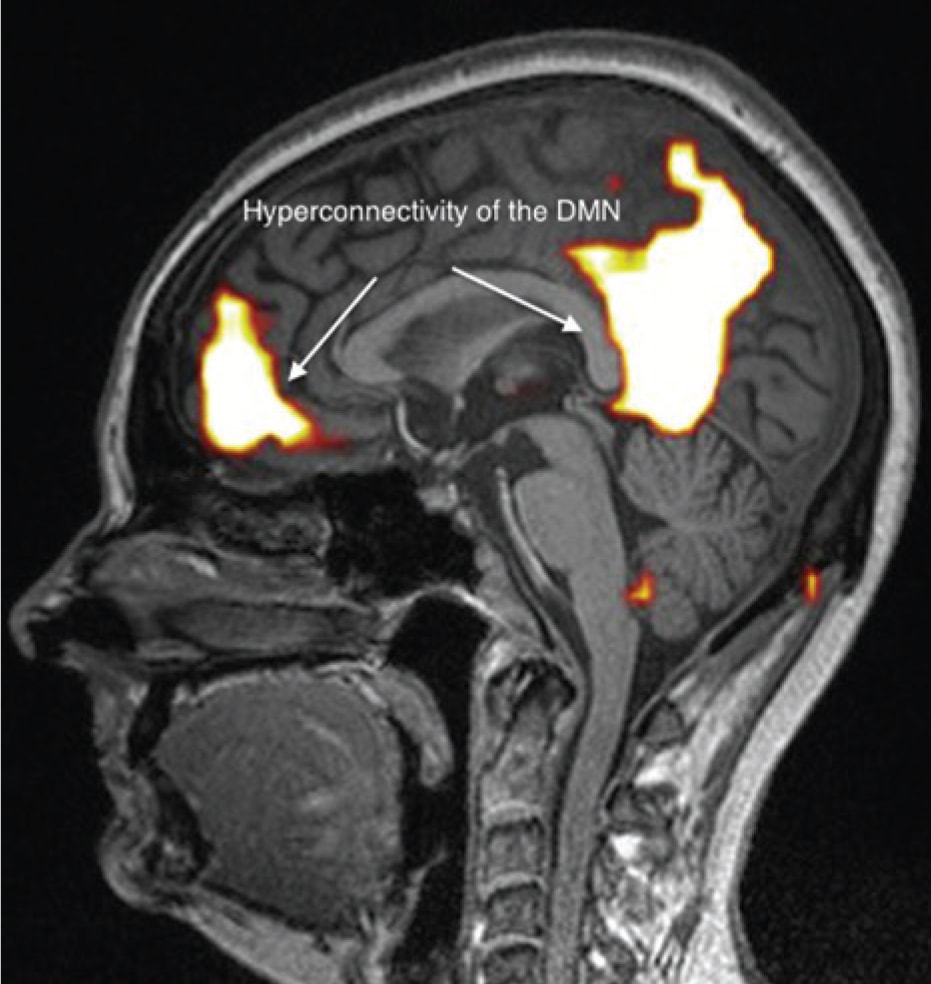
Figure 4: Lateral view of case no. 4.
Case 4. This right handed patient was in her early fifties when tested. Exposure to chemicals started in childhood when she developed double pneumonia, allergies, and eventually asthma. For years before our testing she worked as an air traffic controller, surrounded by cell phone towers at work. In that setting she developed EHS. Her history is negative for head injury. Her past history includes exposure to mold.
The fMRI showed abnormal DMN with hyper connectivity and fragmentation of the anterior component. There was also hyper connectivity of the posterior component.
Case 4. This right handed patient was in her early fifties when tested. Exposure to chemicals started in childhood when she developed double pneumonia, allergies, and eventually asthma. For years before our testing she worked as an air traffic controller, surrounded by cell phone towers at work. In that setting she developed EHS. Her history is negative for head injury. Her past history includes exposure to mold.
The fMRI showed abnormal DMN with hyper connectivity and fragmentation of the anterior component. There was also hyper connectivity of the posterior component.

Figure 5: Lateral view of case no. 5.
Finally there was decreased flow and/or metabolism in the bifrontal lobes diminished flow in the right frontal temporal region was also found (Figure 5).
Finally there was decreased flow and/or metabolism in the bifrontal lobes diminished flow in the right frontal temporal region was also found (Figure 5).
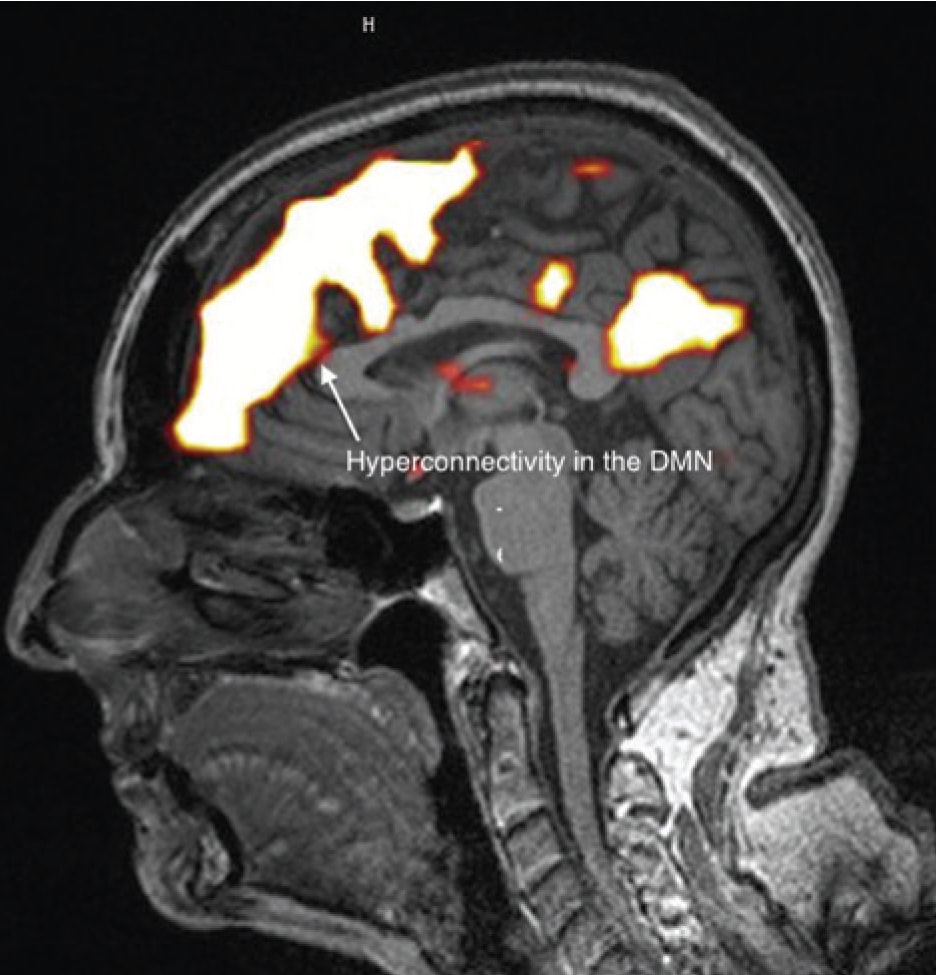
Figure 6: Lateral view of case no. 6.
Case 6. This left handed patient was in her sixties when evaluated. Just a few years before, AT&T constructed a cell phone tower about 500 yards from her home. She developed impaired memory, speech pressure, insomnia, dry eyes and eventually EHS.
Her history is negative for head injury and positive for mold exposure.
The fMRI showed severely abnormal DMN with hyper connectivity of the anterior component (Figure 6).
Case 6. This left handed patient was in her sixties when evaluated. Just a few years before, AT&T constructed a cell phone tower about 500 yards from her home. She developed impaired memory, speech pressure, insomnia, dry eyes and eventually EHS.
Her history is negative for head injury and positive for mold exposure.
The fMRI showed severely abnormal DMN with hyper connectivity of the anterior component (Figure 6).
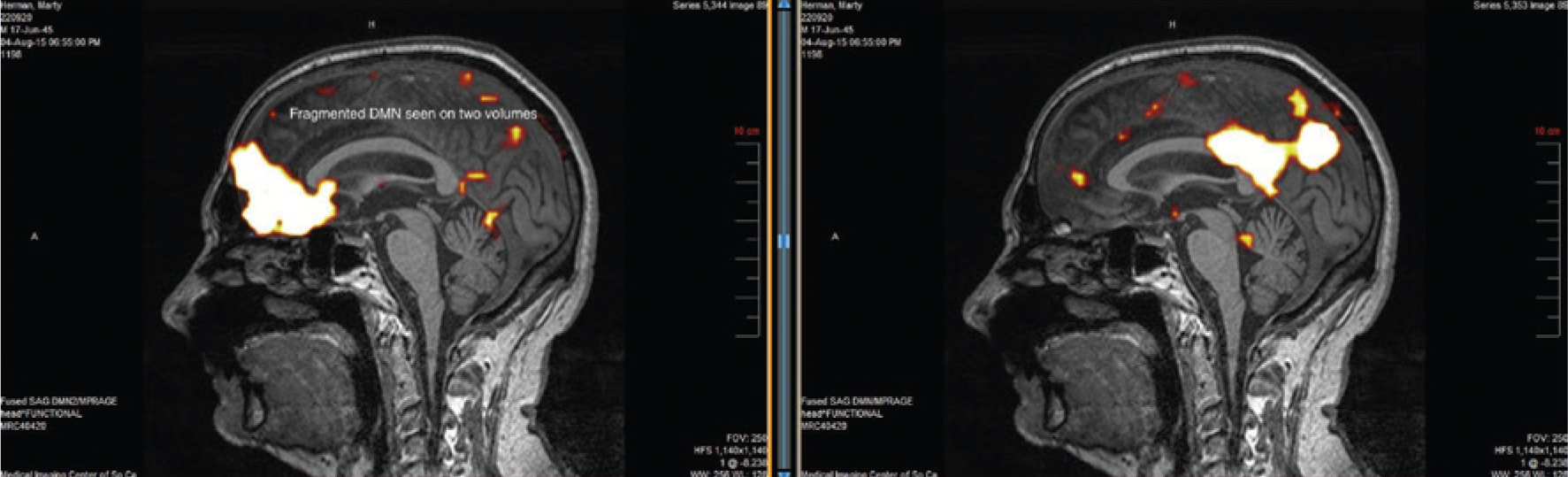
Figure 7: Lateral views of case no. 7.
Case 7. This right handed male was in his seventies when tested. In his work area he had been exposed to EMFs, being surrounded by cell phone towers, many computers, and electrical equipment. He had developed memory and cognitive problems, together with headaches and eventually EHS. Years ago he had been exposed to diesel fumes and more recently to mold. The history is negative for head injury.
The fMRI showed abnormal DMN with fragmentation of the anterior component in the medial orbitofrontal area. It also showed decreased flow and/or metabolism within the bilateral posterior parietal lobes. Finally diffusely decreased white matter tracts in the left cerebral hemisphere were found (Figure 7).
Case 7. This right handed male was in his seventies when tested. In his work area he had been exposed to EMFs, being surrounded by cell phone towers, many computers, and electrical equipment. He had developed memory and cognitive problems, together with headaches and eventually EHS. Years ago he had been exposed to diesel fumes and more recently to mold. The history is negative for head injury.
The fMRI showed abnormal DMN with fragmentation of the anterior component in the medial orbitofrontal area. It also showed decreased flow and/or metabolism within the bilateral posterior parietal lobes. Finally diffusely decreased white matter tracts in the left cerebral hemisphere were found (Figure 7).
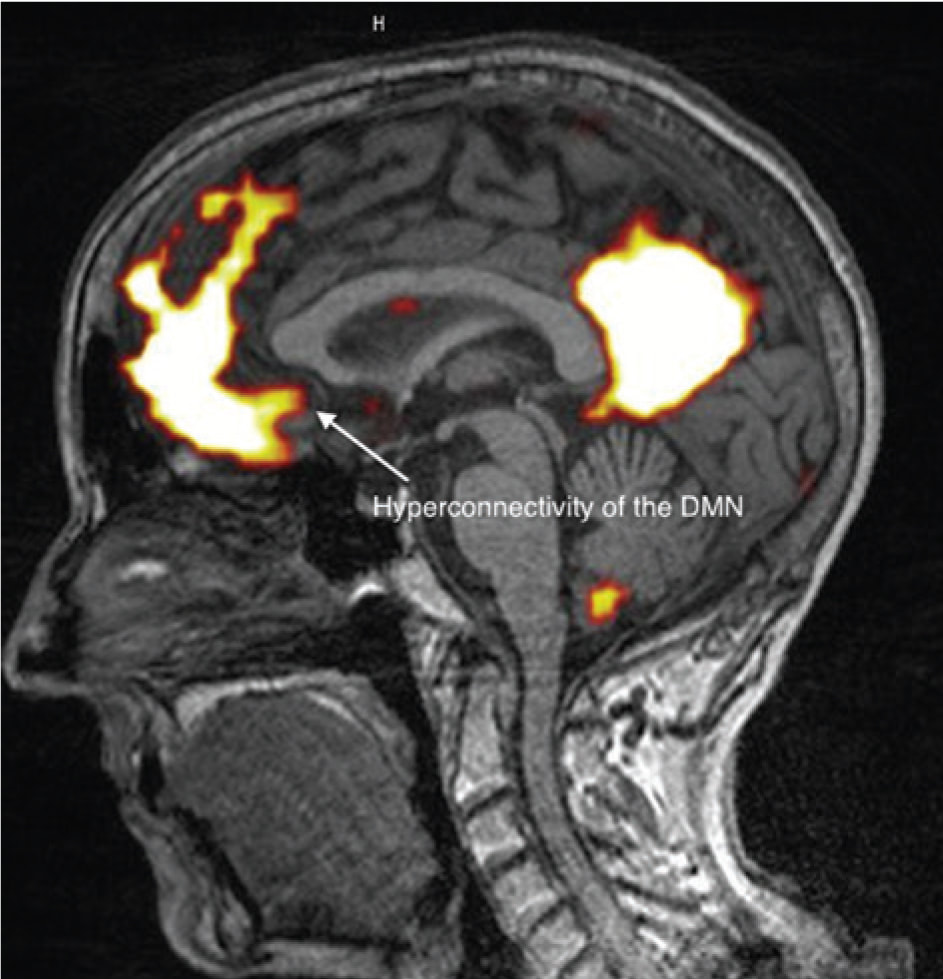
Figure 8: Lateral view of case no. 8.
Case 8. This right handed patient was in her sixties when testing was done. EMF exposure started around 2005 and continued ever since. This continual exposure eventually resulted in the development of EHS. Her complaints included headaches, insomnia, blurred vision, and impairment of speech. Her medical history includes allergies including asthma, mold exposure, and head injuries at ages 10 and 21.
The fMRI showed abnormal DMN with hyper connectivity of the anterior component of the medial orbitofrontal area. Also found was mildly decreased flow and/or metabolism in the bifrontal lobes (arterial spin labeling). Finally there was symmetric loss of white matter tracts in the left posterior parietal lobe (Figure 8).
Case 8. This right handed patient was in her sixties when testing was done. EMF exposure started around 2005 and continued ever since. This continual exposure eventually resulted in the development of EHS. Her complaints included headaches, insomnia, blurred vision, and impairment of speech. Her medical history includes allergies including asthma, mold exposure, and head injuries at ages 10 and 21.
The fMRI showed abnormal DMN with hyper connectivity of the anterior component of the medial orbitofrontal area. Also found was mildly decreased flow and/or metabolism in the bifrontal lobes (arterial spin labeling). Finally there was symmetric loss of white matter tracts in the left posterior parietal lobe (Figure 8).
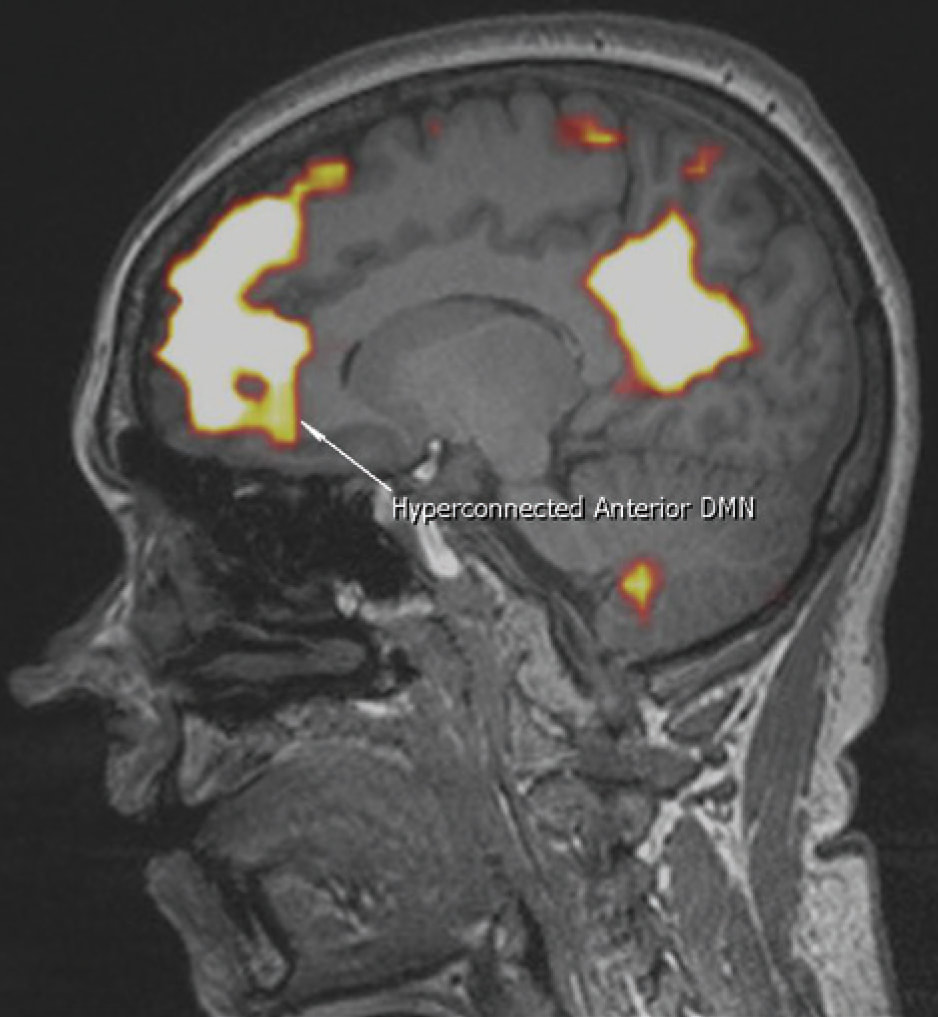
Figure 9: Lateral view of case no. 9.
(A) Sample MRI report for case no. 9. (B) Sample fMRI report for case no. 9.
Case 9. This right handed patient was in her early sixties when evaluated. For more than 20 years she had tested and repaired batteries and was therefore exposed to toxic metals and EMFs on every working day. She was also exposed to a nearby cell phone tower at work.
She developed cognitive and memory impairment, numbness, and eventually EHS and a seizure disorder. Additional medical history included an industrial acci- dent with “electrocution” and also exposure to mold, first at work then at home. Finally her history is positive for head injury.
The fMRI showed a hyperconnected anterior compo- nent of the DMN in the medial orbitofrontal area. Also found was decreased fractional anisotropy in the body of the corpus callosum. Finally there was diminished flow within the bifrontal lobes (Figure 9).
A
MRI OF THE BRAIN HISTORY
Name: DOB: 12/28/1954 Female
Exam Date: 9/8/14
Referring Phys.: GunnarHeuser,M.D.
This is a 59-year-old female with exposure to mold and mercury. The patient has symptoms of seizures, memory loss, and numbness in hands and left arm.
PROCEDURE
Using a 3 Tesla Siemens Verio MRI Open system, the following sequences were obtained:
1) Localizer.
2) T1 3D sagittal MPRAGE.
3) T2 FLAIR sagittal.
4) DWI axial.
5) SWI axial.
6) T2 FLAIR axial. 7) T2 TSE axial.
FINDINGS
No cavum septum pellucidum is seen. No blood products are visualized. There is no diffusion restriction. There is no focal or global volume loss.
The posterior fossa is normal.
The sella and parasellar regions are normal. The flow voids of the vessels of the skull base are identified and normal. The mastoid air cells, paranasal sinuses, and orbits are normal.
There are scattered foci of T2/FLAIR hyperintensity within the supratentorial subcortical white matter located in bifrontal lobes.
IMPRESSION
Scattered foci of T2/FLAIR hyperintensity in the supratentorial subcortical white matter representing gliosis. This can be seen in the setting of prior head trauma, chronic migraine headaches, less likely chronic small vessel ischemic disease given distribution.
B
FUNCTIONAL MRI (fMRI) OF THE BRAIN
HISTORY DOB: 12/28/1954 Female
Exam Date: 9/8/14
Referring Phys.: GunnarHeuser, M.D.
This is a 59-year-old female with exposure to mold and mercury, has symptoms of blackout, seizure, memory loss, head trauma to the left side of brain.
PROCEDURE
Using a 3 Tesla Siemens Verio MRI Open bore system, a functional MRI study was performed using the following sequences:
1) MPRAGE.
2) Resting state network. The EPI sequences for this resting state BOLD scan were then post processed on a
3D workstation and the independent component analysis performed separating out the various networks.
3) Arterial spin labeling.
4) Tractography and fractional anisotropy.
FINDINGS
There is a markedly abnormal default mode network with hyperconnectivity of the anterior component of the default mode. This can be seen in the setting of OCD, chronicpain, post-traumatic brain injury and/ordrug abuse.
The fractional anisotropy is low within the body of the corpus callosum with a minimal value of 0.22 in the anterior body .Diffusion tensor imaging is within normal. The arterial spin labeling demonstrates symmetric diminished flow within bifrontal lobes.
IMPRESSION
1. Abnormal functional MRI with hyperconnected anterior component of the default mode network in the medial orbitofrontal area. This can be seen in the setting of traumatic brain injury, chronic pain, substance abuse and/or OCD.
2. Decreased fractional anisotropy within the body of the corpus callosum with a minimal value of 0.22 in th eanterior body. This is a sign of disorganization of fibers which can be seen in the setting of traumatic brain injury.
3. There is diminished flow within bifrontal regions which is consistent with hypometabolic activity. This can be seen in the setting of traumatic brain injury.
(A) Sample MRI report for case no. 9. (B) Sample fMRI report for case no. 9.
Case 9. This right handed patient was in her early sixties when evaluated. For more than 20 years she had tested and repaired batteries and was therefore exposed to toxic metals and EMFs on every working day. She was also exposed to a nearby cell phone tower at work.
She developed cognitive and memory impairment, numbness, and eventually EHS and a seizure disorder. Additional medical history included an industrial acci- dent with “electrocution” and also exposure to mold, first at work then at home. Finally her history is positive for head injury.
The fMRI showed a hyperconnected anterior compo- nent of the DMN in the medial orbitofrontal area. Also found was decreased fractional anisotropy in the body of the corpus callosum. Finally there was diminished flow within the bifrontal lobes (Figure 9).
A
MRI OF THE BRAIN HISTORY
Name: DOB: 12/28/1954 Female
Exam Date: 9/8/14
Referring Phys.: GunnarHeuser,M.D.
This is a 59-year-old female with exposure to mold and mercury. The patient has symptoms of seizures, memory loss, and numbness in hands and left arm.
PROCEDURE
Using a 3 Tesla Siemens Verio MRI Open system, the following sequences were obtained:
1) Localizer.
2) T1 3D sagittal MPRAGE.
3) T2 FLAIR sagittal.
4) DWI axial.
5) SWI axial.
6) T2 FLAIR axial. 7) T2 TSE axial.
FINDINGS
No cavum septum pellucidum is seen. No blood products are visualized. There is no diffusion restriction. There is no focal or global volume loss.
The posterior fossa is normal.
The sella and parasellar regions are normal. The flow voids of the vessels of the skull base are identified and normal. The mastoid air cells, paranasal sinuses, and orbits are normal.
There are scattered foci of T2/FLAIR hyperintensity within the supratentorial subcortical white matter located in bifrontal lobes.
IMPRESSION
Scattered foci of T2/FLAIR hyperintensity in the supratentorial subcortical white matter representing gliosis. This can be seen in the setting of prior head trauma, chronic migraine headaches, less likely chronic small vessel ischemic disease given distribution.
B
FUNCTIONAL MRI (fMRI) OF THE BRAIN
HISTORY DOB: 12/28/1954 Female
Exam Date: 9/8/14
Referring Phys.: GunnarHeuser, M.D.
This is a 59-year-old female with exposure to mold and mercury, has symptoms of blackout, seizure, memory loss, head trauma to the left side of brain.
PROCEDURE
Using a 3 Tesla Siemens Verio MRI Open bore system, a functional MRI study was performed using the following sequences:
1) MPRAGE.
2) Resting state network. The EPI sequences for this resting state BOLD scan were then post processed on a
3D workstation and the independent component analysis performed separating out the various networks.
3) Arterial spin labeling.
4) Tractography and fractional anisotropy.
FINDINGS
There is a markedly abnormal default mode network with hyperconnectivity of the anterior component of the default mode. This can be seen in the setting of OCD, chronicpain, post-traumatic brain injury and/ordrug abuse.
The fractional anisotropy is low within the body of the corpus callosum with a minimal value of 0.22 in the anterior body .Diffusion tensor imaging is within normal. The arterial spin labeling demonstrates symmetric diminished flow within bifrontal lobes.
IMPRESSION
1. Abnormal functional MRI with hyperconnected anterior component of the default mode network in the medial orbitofrontal area. This can be seen in the setting of traumatic brain injury, chronic pain, substance abuse and/or OCD.
2. Decreased fractional anisotropy within the body of the corpus callosum with a minimal value of 0.22 in th eanterior body. This is a sign of disorganization of fibers which can be seen in the setting of traumatic brain injury.
3. There is diminished flow within bifrontal regions which is consistent with hypometabolic activity. This can be seen in the setting of traumatic brain injury.
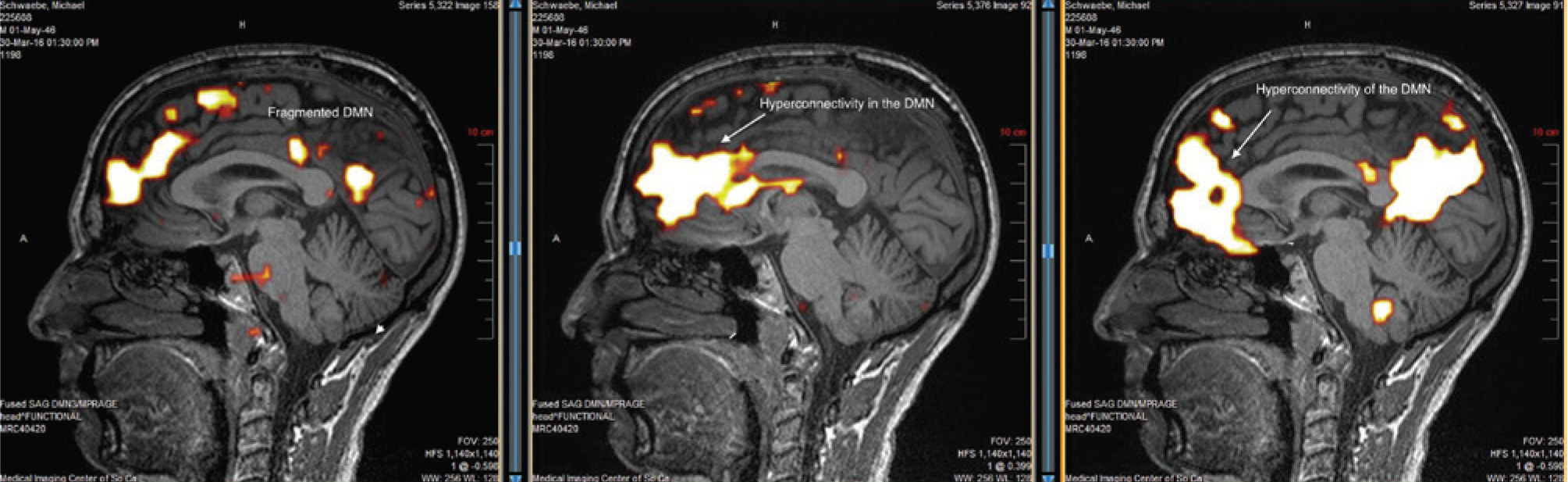
Figure 10: Lateral views of case no. 10
Case 10. This right handed patient was in his sixties when testing was done. Over the years he had been exposed to pesticides and to mold. He had experienced a concussion about 10 years earlier. He gradually developed EHS. The fMRI showed abnormal DMN with fragmentation and hyper connectivity of the anterior component of the default mode in the medial orbitofrontal area. There was borderline decreased flow and/or metabolism within bifrontal lobes (Figure 10).
Discussion
More than 30 years ago we became interested in the effects of toxic chemical exposure on the brain. We selected more than 70 patients who had developed multi system complaints after long-term exposure to potentially neurotoxic chemicals. All patients underwent functional brain scans of the SPECT type. They were all abnormal and statistically analyzed. The results were published [1] in a peer reviewed journal with the conclusion that neurotoxic chemical exposure can lead to long-term effects including abnormalities in brain function. The abnormalities seen were still present years after toxic exposure had ceased. The potentially neurotoxic effects of chemicals were further discussed in a German publication [3].
Since some of our patients had developed exquisite sensitivity to even small amounts of chemicals we decided to document brain function in these patients with multiple chemical sensitivity (MCS). For this study we chose positron emission tomography (PET) scanning of the brain and found definite objective abnormalities in these patients. The results were published with the conclusion that patients with MCS have objective abnormalities in brain function [2]. It should be noted that a number of PET studies were published by other authors but did not address MCS [4–7].
Of interest was the fact that PET brain scans in MCS patients showed increased activity in the amygdala [2]. This structure is known to control emotions. This is why some patients with MCS develop an emotional disorder which can be explained on the basis of a “hot” amygdala. In view of this past finding with our MCS patients we believe that EHS patients should be studied with PET scans so as to find out whether their amygdalae are also hyperactive.
MCS was further discussed in a consensus paper in which GH was a co-author [8].
In more recent years we started seeing patients who claimed exquisite sensitivity to electromagnetic fields (electrohypersensitivity, commonly recognized as EHS). It was very interesting to find that the complaints these patients had developed were similar to the complaints patients had who were exposed to and sensitive to chemicals: headaches, cognitive and memory problems, intermittent problems with balance, and intermittent tremor. This syndrome has been described by Carpenter and others [9–12].
The late Dr. Ross Adey [13] found that chemicals and EMFs can interact and aggravate each others’ effects. This became a finding we confirmed in our patients.
We suggested to some of our patients with EHS that they undergo a functional brain scan to document potential abnormalities. They agreed but did not want to have any radioactive material used for the scan. This of course excluded PET and SPECT scanning of the brain. Since these patients had significant complaints and were at times disabled we felt that it was important to obtain a functional MRI (fMRI) to document poten- tial abnormalities of brain function. In the beginning this was considered as medically necessary and was not a research project and therefore not funded by any agency. Since insurance coverage is not yet available for fMRI, patients had to cover the cost of the whole evaluation. While fMRI studies look at functional connections between some brain areas, no studies in the literature specifically addressed functional connectivity after exposure to EMF. However, some studies in the literature refer to connections between specific areas of the brain by measuring EEG and related activities. None of these studies have addressed patients with EHS.
Conclusion
All fMRI brain scans were abnormal in our patients. Their abnormalities were very similar in all of them.
The study of fMRI created a new language which had to be learned. We have included some references which help the reader to understand this new terminology [17–21].
The question now arises whether the same abnormalities seen in all 10 patients can become a diagnostic aid or biomarker for determining whether or not a patient has electrohypersensitivity (EHS). Some researchers have claimed that a diagnosis of EHS should really be a psychi- atric diagnosis [22]. Other researchers have attempted to measure EHS [23]. The possible psychiatric aspects of EHS remind us of the history of medicine when epilepsy was considered to be a diagnosis of possession by the devil [24]. It was only the discovery of the EEG which helped to find epilepsy to be a real disease with objective findings. We hope that fMRI will play the role of the EEG in EHS.
In the context of the above paragraph we should mention the articles by Belpomme et al. [25] and De Luca et al. [26] which suggest a long list of biomarkers for the diagnosis of EHS. This list does not include functional brain scans as potential biomarkers.
The treatment of EHS is very difficult. It was reviewed in a recent publication [27]. We have found that hyperbaric oxygen is at times helpful [28]. We have proposed that every patient with EHS should be checked for mast cell disease since mast cell abnormalities were found by Gangi and Johansson [29]. We described mast cell disor- der in patients with MCS [30]. Also we found mast cell disorder in some of our patients with EHS [31]. Finally we believe that mold and mold toxin (mycotoxin) exposure can trigger EHS. Mast cell disease and mold problems are treatable. Their treatment may decrease EHS. Otherwise treatment consists basically of avoidance.
A final point of interest is the fact that the abnormal- ity seen on the fMRI can also be seen after head injury [32, 33]. Indeed, many of our patients complaining of EHS have a history of head injury (see our case reports).
Since neurotoxic chemicals as well as head injury and EMF exposure are known to impair the blood brain barrier, it is almost to be expected that singly or in combination they make a given patient more vulnerable to impaired brain function (including seizures).
In the past we studied patients who had developed multi system complaints after exposure to a number of neurotoxins. The only patients who developed a seizure disorder were the ones who gave a history of past head injury [31]. Two of our patients (#3 and 9) developed a well
documented seizure disorder. This can be understood as having been “kindled” by repeated exposures to EMFs.
Our study needs to be enlarged and also duplicated by others. The subject will be of increasing importance in our society in which we and our children are all exposed to more and more EMFs.
Acknowledgements: Medical Imaging of Southern California graciously made their studies (MRI and fMRI) available at a significant discount. We also acknowledge Brea Blevins who helped to retrieve and to display the images published in this paper. Most patients were either self referred or referred by their physician. Some were referred by The Peoples Initiative Foundation which was formed and is directed by Elizabeth Barris.
Author Statement
Research funding: No funds for this study were available from any foundation or other financial entity for this study. Partial payment was received for two patient studies by a charitable foundation (The Peoples Initiative Foundation). Patients paid for their own consultations and testing. No insurance reimbursements were available for the fMRI study. Conflict of interest: Authors state no conflict of interest. Informed consent: Informed consent has been obtained from all individuals. Ethical approval: Ethical approval was not applicable.
References
1. Heuser G, Mena I. Neurospect in neurotoxic chemical exposure.Demonstration of long-term functional abnormalities. Toxicol Ind Health 1998;14(6):813–27.
2. Heuser G, Wu JC. Deep subcortical (including limbic) hypermetabolism in patients with chemical intolerance: human PET studies. Ann N Y Acad Sci 2001;933:319–22.
3. Heuser G. Functional brain Imaging with SPECT and PET after neurotoxic exposure: two and three-dimensional displays. Zeitschrift fur Umweltmedizin 1999;8:284–5.
4. Huber R, Treyer V, Schuderer J, Berthold T, Buck A, et al. Exposure to pulse-modulated radio frequency electromagnetic fields affects regional cerebral blood flow. Eur J Neurosci 2005;21(4):1000–6.
5. Aalto S, Haarala C, Brück A, Sipilä H, Hämäläinen H, et al. Mobile phone affects cerebral blood flow in humans. J Cereb Blood Flow Metab 2006;26(7):885–90.
6. Haarala C, Aalto S, Hautzel H, Julkunen L, Rinne JO, et al. Effects of a 902 MHz mobile phone on cerebral blood flow in humans: a PET study. Neuroreport. 2003;14(16):2019–23.
7. Huber R, Treyer V, Borbély AA, Schuderer J, Gottselig JM, et al. Electromagnetic fields, such as those from mobile phones, alter regional cerebral blood flow and sleep and waking EEG. J Sleep Res 2002;11(4):289–95.
8. Bartha L. Multiple chemical sensitivity: a 1999 consensus. Arch Environ Health 1999;54(3):147–9.
9. Carpenter DO. The microwave syndrome or electrohypersensitivity: historical background. Rev Environ Health 2015;30(4):217–22.
10. Hedendahl L, Carlberg M, Hardell L. Electromagnetic hypersensitivity – an increasing challenge to the medical profession. Rev Environ Health 2015;30(4):209–15.
11. Genuis SJ, Lipp CT. Electromagnetic hypersensitivity: fact or fiction? Sci Total Environ 2012;414:103–12.
12. McCarty DE, Carrubba S, Chesson AL, Frilot C, Gonzalez-Toledo E, et al. Electromagnetic hypersensitivity: evidence for a novel neurological syndrome. Int J Neurosci 2011;121(12):670–6.
13. Adey WR. Joint actions of environmental nonionizing electromagnetic fields and chemical pollution in cancer promotion. Environ Health Perspect 1990;86:297–305.
14. Haarala C, Takio F, Rintee T, Laine M, Koivisto M, et al. Pulsed and continuous wave mobile phone exposure over left versus right hemisphere: effects on human cognitive function. Bioelec- tromagnetics 2007;28(4):289–95.
15. Vecchio F, Babiloni C, Ferreri F, Curcio G, Fini R, et al. Mobile phone emission modulates interhemispheric functional coupling of EEG alpha rhythms. Eur J Neurosci 2007;25(6):1908–13.
16. Yang L, Chen Q, Lv B, Wu T. Long-Term evolution electromagnetic fields exposure modulates the resting state EEG on alpha and beta bands. Clin EEG Neurosci 2017;48(3):168–75.
17. van den Heuvel MP, Hulshoff Pol HE. Exploring the brain net- work: a review on resting-state fMRI functional connectivity. Eur Neuropsychopharmacol 2010;20(8):519–34.
18. Horn A, Dirk O, Reisert M, Blankenburg F. Default Mode Network. [revised 2016 August]. In: Wikipedia [Internet]. San Francisco, CA: NeuroImage; 2006 September. 10 pages. Available from: www.wikipedia.com. DOI: 10.1016.
19. Liston C, Chen AC, Zebley BD, Drysdale AT, Gordon R, et al.
Default mode network mechanisms of transcranial magneticstimulation in depression. Biol Psychiatry 2014;76(7):517–26.
20. Smith SM, Vidaurre D, Beckmann CF, Glasser MF, Jenkinson M, et al. Functional connectomics from resting-state fMRI. Trends Cogn Sci 2013;17(12):666–82.
21. Lee MH, Smyser CD, Shimony JS. Resting-state fMRI: a review of methods and clinical applications. AJNR Am J Neuroradiol 2013;34(10):1866–72.
22. Rubin G J, Hillert L, Nieto-Hernandez R, van Rongen E, Oftedal G. Do people with idiopathic environmental intolerance attributed to electromagnetic fields display physiological effects when exposed to electromagnetic fields? A systematic review of provocation studies Bioelectromagnetics 2011;32(8):593–609.
23. Tuengler A, von Klitzing L. Hypothesis on how to measure electromagnetic hypersensitivity. Electromagn Biol Med 2013;32(3):281–90.
24. Espí Forcén C, Espí Forcén F. Demonic possessions and mental illness: discussion of selected cases in late medieval hagiographical literature. Early Sci Med 2014;19(3):258–79.
25. Belpomme D, Campagnac C, Irigaray P. Reliable disease biomarkers characterizing and identifying electrohypersensi- tivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev Environ Health
2015;30(4):251–71.
26. De Luca C, Chung Sheun Thai J, Raskovic D, Cesareo E, Caccamo D, et al. Metabolic and genetic screening of electromagnetic hypersensitive subjects as a feasible tool for diagnostics and intervention. Mediators Inflamm 2014;2014:924184.
27. Rubin GJ, Das Munshi J, Wessely S. A systematic review of treatments for electromagnetic hypersensitivity. Psychother Psychosom 2006;75(1):12–8.
28. Heuser G, Uszler JM. Hyperbaric oxygenation for cerebral palsy.Lancet 2001;357(9273):2053–4. Erratum in: Lancet 2001 Nov 24;358(9295):1820.
29. Gangi S, Johansson O. A theoretical model based upon mast cells and histamine to explain the recently proclaimed sensitivity to electric and/or magnetic fields in humans. Med Hypotheses 2000;54(4):663–71.
30. Heuser G. Mast cell disorder to be ruled out in MCS. Arch Environ Health 2000;55(4):284–5.
31. Unpublished observations by authors.
32. Mishra AM, Bai X, Sanganahalli BG, Waxman SG, Shatillo O, et al. Decreased resting functional connectivity after traumatic brain injury in the rat. Plos One 2014;09(4):e95280.
33. Zhou Y, Milham M, Lui Y, Zhou Y, Milham MP, et al. Default-mode network disruption in mild traumatic brain injury. Radiology 2012;265(3):882–92.
Case 10. This right handed patient was in his sixties when testing was done. Over the years he had been exposed to pesticides and to mold. He had experienced a concussion about 10 years earlier. He gradually developed EHS. The fMRI showed abnormal DMN with fragmentation and hyper connectivity of the anterior component of the default mode in the medial orbitofrontal area. There was borderline decreased flow and/or metabolism within bifrontal lobes (Figure 10).
Discussion
More than 30 years ago we became interested in the effects of toxic chemical exposure on the brain. We selected more than 70 patients who had developed multi system complaints after long-term exposure to potentially neurotoxic chemicals. All patients underwent functional brain scans of the SPECT type. They were all abnormal and statistically analyzed. The results were published [1] in a peer reviewed journal with the conclusion that neurotoxic chemical exposure can lead to long-term effects including abnormalities in brain function. The abnormalities seen were still present years after toxic exposure had ceased. The potentially neurotoxic effects of chemicals were further discussed in a German publication [3].
Since some of our patients had developed exquisite sensitivity to even small amounts of chemicals we decided to document brain function in these patients with multiple chemical sensitivity (MCS). For this study we chose positron emission tomography (PET) scanning of the brain and found definite objective abnormalities in these patients. The results were published with the conclusion that patients with MCS have objective abnormalities in brain function [2]. It should be noted that a number of PET studies were published by other authors but did not address MCS [4–7].
Of interest was the fact that PET brain scans in MCS patients showed increased activity in the amygdala [2]. This structure is known to control emotions. This is why some patients with MCS develop an emotional disorder which can be explained on the basis of a “hot” amygdala. In view of this past finding with our MCS patients we believe that EHS patients should be studied with PET scans so as to find out whether their amygdalae are also hyperactive.
MCS was further discussed in a consensus paper in which GH was a co-author [8].
In more recent years we started seeing patients who claimed exquisite sensitivity to electromagnetic fields (electrohypersensitivity, commonly recognized as EHS). It was very interesting to find that the complaints these patients had developed were similar to the complaints patients had who were exposed to and sensitive to chemicals: headaches, cognitive and memory problems, intermittent problems with balance, and intermittent tremor. This syndrome has been described by Carpenter and others [9–12].
The late Dr. Ross Adey [13] found that chemicals and EMFs can interact and aggravate each others’ effects. This became a finding we confirmed in our patients.
We suggested to some of our patients with EHS that they undergo a functional brain scan to document potential abnormalities. They agreed but did not want to have any radioactive material used for the scan. This of course excluded PET and SPECT scanning of the brain. Since these patients had significant complaints and were at times disabled we felt that it was important to obtain a functional MRI (fMRI) to document poten- tial abnormalities of brain function. In the beginning this was considered as medically necessary and was not a research project and therefore not funded by any agency. Since insurance coverage is not yet available for fMRI, patients had to cover the cost of the whole evaluation. While fMRI studies look at functional connections between some brain areas, no studies in the literature specifically addressed functional connectivity after exposure to EMF. However, some studies in the literature refer to connections between specific areas of the brain by measuring EEG and related activities. None of these studies have addressed patients with EHS.
Conclusion
All fMRI brain scans were abnormal in our patients. Their abnormalities were very similar in all of them.
The study of fMRI created a new language which had to be learned. We have included some references which help the reader to understand this new terminology [17–21].
The question now arises whether the same abnormalities seen in all 10 patients can become a diagnostic aid or biomarker for determining whether or not a patient has electrohypersensitivity (EHS). Some researchers have claimed that a diagnosis of EHS should really be a psychi- atric diagnosis [22]. Other researchers have attempted to measure EHS [23]. The possible psychiatric aspects of EHS remind us of the history of medicine when epilepsy was considered to be a diagnosis of possession by the devil [24]. It was only the discovery of the EEG which helped to find epilepsy to be a real disease with objective findings. We hope that fMRI will play the role of the EEG in EHS.
In the context of the above paragraph we should mention the articles by Belpomme et al. [25] and De Luca et al. [26] which suggest a long list of biomarkers for the diagnosis of EHS. This list does not include functional brain scans as potential biomarkers.
The treatment of EHS is very difficult. It was reviewed in a recent publication [27]. We have found that hyperbaric oxygen is at times helpful [28]. We have proposed that every patient with EHS should be checked for mast cell disease since mast cell abnormalities were found by Gangi and Johansson [29]. We described mast cell disor- der in patients with MCS [30]. Also we found mast cell disorder in some of our patients with EHS [31]. Finally we believe that mold and mold toxin (mycotoxin) exposure can trigger EHS. Mast cell disease and mold problems are treatable. Their treatment may decrease EHS. Otherwise treatment consists basically of avoidance.
A final point of interest is the fact that the abnormal- ity seen on the fMRI can also be seen after head injury [32, 33]. Indeed, many of our patients complaining of EHS have a history of head injury (see our case reports).
Since neurotoxic chemicals as well as head injury and EMF exposure are known to impair the blood brain barrier, it is almost to be expected that singly or in combination they make a given patient more vulnerable to impaired brain function (including seizures).
In the past we studied patients who had developed multi system complaints after exposure to a number of neurotoxins. The only patients who developed a seizure disorder were the ones who gave a history of past head injury [31]. Two of our patients (#3 and 9) developed a well
documented seizure disorder. This can be understood as having been “kindled” by repeated exposures to EMFs.
Our study needs to be enlarged and also duplicated by others. The subject will be of increasing importance in our society in which we and our children are all exposed to more and more EMFs.
Acknowledgements: Medical Imaging of Southern California graciously made their studies (MRI and fMRI) available at a significant discount. We also acknowledge Brea Blevins who helped to retrieve and to display the images published in this paper. Most patients were either self referred or referred by their physician. Some were referred by The Peoples Initiative Foundation which was formed and is directed by Elizabeth Barris.
Author Statement
Research funding: No funds for this study were available from any foundation or other financial entity for this study. Partial payment was received for two patient studies by a charitable foundation (The Peoples Initiative Foundation). Patients paid for their own consultations and testing. No insurance reimbursements were available for the fMRI study. Conflict of interest: Authors state no conflict of interest. Informed consent: Informed consent has been obtained from all individuals. Ethical approval: Ethical approval was not applicable.
References
1. Heuser G, Mena I. Neurospect in neurotoxic chemical exposure.Demonstration of long-term functional abnormalities. Toxicol Ind Health 1998;14(6):813–27.
2. Heuser G, Wu JC. Deep subcortical (including limbic) hypermetabolism in patients with chemical intolerance: human PET studies. Ann N Y Acad Sci 2001;933:319–22.
3. Heuser G. Functional brain Imaging with SPECT and PET after neurotoxic exposure: two and three-dimensional displays. Zeitschrift fur Umweltmedizin 1999;8:284–5.
4. Huber R, Treyer V, Schuderer J, Berthold T, Buck A, et al. Exposure to pulse-modulated radio frequency electromagnetic fields affects regional cerebral blood flow. Eur J Neurosci 2005;21(4):1000–6.
5. Aalto S, Haarala C, Brück A, Sipilä H, Hämäläinen H, et al. Mobile phone affects cerebral blood flow in humans. J Cereb Blood Flow Metab 2006;26(7):885–90.
6. Haarala C, Aalto S, Hautzel H, Julkunen L, Rinne JO, et al. Effects of a 902 MHz mobile phone on cerebral blood flow in humans: a PET study. Neuroreport. 2003;14(16):2019–23.
7. Huber R, Treyer V, Borbély AA, Schuderer J, Gottselig JM, et al. Electromagnetic fields, such as those from mobile phones, alter regional cerebral blood flow and sleep and waking EEG. J Sleep Res 2002;11(4):289–95.
8. Bartha L. Multiple chemical sensitivity: a 1999 consensus. Arch Environ Health 1999;54(3):147–9.
9. Carpenter DO. The microwave syndrome or electrohypersensitivity: historical background. Rev Environ Health 2015;30(4):217–22.
10. Hedendahl L, Carlberg M, Hardell L. Electromagnetic hypersensitivity – an increasing challenge to the medical profession. Rev Environ Health 2015;30(4):209–15.
11. Genuis SJ, Lipp CT. Electromagnetic hypersensitivity: fact or fiction? Sci Total Environ 2012;414:103–12.
12. McCarty DE, Carrubba S, Chesson AL, Frilot C, Gonzalez-Toledo E, et al. Electromagnetic hypersensitivity: evidence for a novel neurological syndrome. Int J Neurosci 2011;121(12):670–6.
13. Adey WR. Joint actions of environmental nonionizing electromagnetic fields and chemical pollution in cancer promotion. Environ Health Perspect 1990;86:297–305.
14. Haarala C, Takio F, Rintee T, Laine M, Koivisto M, et al. Pulsed and continuous wave mobile phone exposure over left versus right hemisphere: effects on human cognitive function. Bioelec- tromagnetics 2007;28(4):289–95.
15. Vecchio F, Babiloni C, Ferreri F, Curcio G, Fini R, et al. Mobile phone emission modulates interhemispheric functional coupling of EEG alpha rhythms. Eur J Neurosci 2007;25(6):1908–13.
16. Yang L, Chen Q, Lv B, Wu T. Long-Term evolution electromagnetic fields exposure modulates the resting state EEG on alpha and beta bands. Clin EEG Neurosci 2017;48(3):168–75.
17. van den Heuvel MP, Hulshoff Pol HE. Exploring the brain net- work: a review on resting-state fMRI functional connectivity. Eur Neuropsychopharmacol 2010;20(8):519–34.
18. Horn A, Dirk O, Reisert M, Blankenburg F. Default Mode Network. [revised 2016 August]. In: Wikipedia [Internet]. San Francisco, CA: NeuroImage; 2006 September. 10 pages. Available from: www.wikipedia.com. DOI: 10.1016.
19. Liston C, Chen AC, Zebley BD, Drysdale AT, Gordon R, et al.
Default mode network mechanisms of transcranial magneticstimulation in depression. Biol Psychiatry 2014;76(7):517–26.
20. Smith SM, Vidaurre D, Beckmann CF, Glasser MF, Jenkinson M, et al. Functional connectomics from resting-state fMRI. Trends Cogn Sci 2013;17(12):666–82.
21. Lee MH, Smyser CD, Shimony JS. Resting-state fMRI: a review of methods and clinical applications. AJNR Am J Neuroradiol 2013;34(10):1866–72.
22. Rubin G J, Hillert L, Nieto-Hernandez R, van Rongen E, Oftedal G. Do people with idiopathic environmental intolerance attributed to electromagnetic fields display physiological effects when exposed to electromagnetic fields? A systematic review of provocation studies Bioelectromagnetics 2011;32(8):593–609.
23. Tuengler A, von Klitzing L. Hypothesis on how to measure electromagnetic hypersensitivity. Electromagn Biol Med 2013;32(3):281–90.
24. Espí Forcén C, Espí Forcén F. Demonic possessions and mental illness: discussion of selected cases in late medieval hagiographical literature. Early Sci Med 2014;19(3):258–79.
25. Belpomme D, Campagnac C, Irigaray P. Reliable disease biomarkers characterizing and identifying electrohypersensi- tivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev Environ Health
2015;30(4):251–71.
26. De Luca C, Chung Sheun Thai J, Raskovic D, Cesareo E, Caccamo D, et al. Metabolic and genetic screening of electromagnetic hypersensitive subjects as a feasible tool for diagnostics and intervention. Mediators Inflamm 2014;2014:924184.
27. Rubin GJ, Das Munshi J, Wessely S. A systematic review of treatments for electromagnetic hypersensitivity. Psychother Psychosom 2006;75(1):12–8.
28. Heuser G, Uszler JM. Hyperbaric oxygenation for cerebral palsy.Lancet 2001;357(9273):2053–4. Erratum in: Lancet 2001 Nov 24;358(9295):1820.
29. Gangi S, Johansson O. A theoretical model based upon mast cells and histamine to explain the recently proclaimed sensitivity to electric and/or magnetic fields in humans. Med Hypotheses 2000;54(4):663–71.
30. Heuser G. Mast cell disorder to be ruled out in MCS. Arch Environ Health 2000;55(4):284–5.
31. Unpublished observations by authors.
32. Mishra AM, Bai X, Sanganahalli BG, Waxman SG, Shatillo O, et al. Decreased resting functional connectivity after traumatic brain injury in the rat. Plos One 2014;09(4):e95280.
33. Zhou Y, Milham M, Lui Y, Zhou Y, Milham MP, et al. Default-mode network disruption in mild traumatic brain injury. Radiology 2012;265(3):882–92.
 RSS Feed
RSS Feed
